
Архив офтальмологии Украины Том 13, №2, 2025
Вернуться к номеру
Особливості клінічного перебігу невриту зорового нерва внаслідок сфеноїдиту
Авторы: Євчев Ф.Д., Єпішева С.М., Дьячкова З.Є., Терещенко А.А.
Одеський національний медичний університет, м. Одеса, Україна
Рубрики: Офтальмология
Разделы: Справочник специалиста
Версия для печати
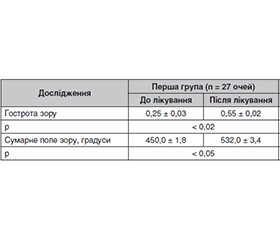
Актуальність. Неврит зорового нерва є найчастішою причиною ушкодження зорового нерва в осіб молодого віку і відрізняється різноманіттям етіологічних факторів, включно з інфекційними, автоімунними й демієлінізуючими захворюваннями. Мета: визначити особливості клінічного перебігу невриту зорового нерва внаслідок сфеноїдиту. Матеріали та методи. Обстежено 35 пацієнтів віком від 18 до 52 років з діагнозом невриту зорового нерва, середній вік хворих — 31,2 ± 15,7 року. Пацієнтів було рандомізовано на дві групи: перша група — 27 хворих (27 очей) — отримувала системну протизапальну, імуносупресивну, десенсибілізуючу терапію, електрофорез антибактеріальних речовин, а пацієнтам другої групи — 8 хворих (8 очей), у яких було діагностовано запалення зорового нерва на тлі сфеноїдиту, окрім означеної терапії виконували ендоназальний електрофорез антибактеріального, антисептичного засобу з використанням кортикостероїдних і антигістамінних препаратів. Проводилося загальноклінічне обстеження, визначення гостроти зору, поля зору, офтальмоскопія, комп’ютерна томографія, передня і задня риноскопія, фарингоскопія, рентгеноскопія в прямих проєкціях і прицільній боковій проєкції, ендоскопія. Результати. У хворих на неврит зорового нерва на тлі сфеноїдиту на фоні загальної протизапальної терапії були купіровані запальні ознаки захворювання (зник головний біль, біль при натисканні в зоні носа, поліпшилися носове дихання і нюх тощо), підвищилася гострота зору (р < 0,02) і відбулося розширення сумарного поля зору (р < 0,05). Частіше пацієнти скаржилися на головний біль у зоні скроні й потилиці та при нахилі голови вперед, ускладнення дихання і виділення з носа, слабкість, підвищення температури й погіршення зору. Висновки. Одними з клінічних диференціальних показників при діагностиці невриту зорового нерва на тлі сфеноїдиту можуть стати головний біль, біль при натисканні в зоні носа, погіршення носового дихання й нюху. Діагностику невриту зорового нерва необхідно виконувати офтальмологу сумісно з оториноларингологом, використовуючи променеві методи діагностики, риноскопію, фарингоскопію. Ми рекомендуємо для лікування хворих на запалення зорового нерва на тлі сфеноїдиту використовувати вакуумне промивання носових порожнин і ендоназальний електрофорез антибактеріальних, антисептичних та десенсибілізуючих препаратів на фоні загальної протизапальної терапії.
Background. Optic neuritis is the most common cause of optic nerve damage in young people and is characterized by a variety of etiological factors, including infectious, autoimmune, and demyelinating diseases. Objective: to determine the features of the clinical course of optic neuritis due to sphenoiditis. Materials and methods. We examined 35 patients aged 18 to 52 years with a diagnosis of optic neuritis, their average age was 31.2 ± 15.7 years. Patients were randomized into two groups. The first group of 27 patients (27 eyes) received systemic anti-inflammatory, immunosuppressive, desensitizing therapy, electrophoresis of antibacterial substances. In the second group of 8 patients (8 eyes), who were diagnosed with inflammation of the optic nerve on the background of sphenoiditis, in addition to the indicated therapy, endonasal electrophoresis of an antibacterial, antiseptic agent was conducted, using corticosteroid and antihistamine drugs. A general ophthalmic examination was done along with determination of visual acuity, visual fields, ophthalmoscopy, computed tomography, anterior and posterior rhinoscopy, pharyngoscopy, fluoroscopy in direct and targeted lateral projections, endoscopy. Results. In patients with optic neuritis on the background of sphenoiditis, the inflammatory symptoms of the disease (headache, pain when pressing in the nose area disappeared, nasal breathing and smell improved) were relieved, visual acuity increased (p < 0.02) and the total visual field expanded (p < 0.05) following general anti-inflammatory therapy. More often, patients complained of headache in the temple and occipital area and when tilting the head forward, difficulty breathing and nasal discharge, weakness, fever and deterioration of vision. Conclusions. One of the clinical differential indicators in the diagnosis of optic neuritis on the background of sphenoiditis can be headaches, pain when pressing in the nose area, deterioration of nasal breathing and smell. Diagnosis of optic neuritis should be performed by an ophthalmologist in conjunction with an otorhinolaryngologist, using radiological methods, rhinoscopy, pharyngoscopy. It is recommended to use vacuum lavage of the nasal cavities and endonasal electrophoresis of antibacterial, antiseptic and desensitizing drugs against the background of general anti-inflammatory therapy for the management of patients with optic neuritis due to sphenoiditis.
неврит зорового нерва; приносові пазухи; сфеноїдит; запалення
optic neuritis; accessory sinuses; sphenoiditis; inflammation
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Jin YP, de Pedro-Cuesta J, Soderstrom M, Link H. Incidence of optic neuritis in Stockholm, Sweden, 1990–1995: II. Time and space patterns. Arch Neurol. 1999;56:975-980.
- Soelberg K, Jarius S, Skejoe H, Engberg H et al. A po–pulation-based prospective study of optic neuritis. Mult Scler. 2017;23:1893-1901.
- Asseyer S et al. The Acute Optic Neuritis Network (ACON): Study protocol of a non-interventional prospective multicenter study on diagnosis and treatment of acute optic neuritis. Frontiers in Neurology. 2023 Feb 24;14:1102353. doi: 10.3389/fneur.2023.1102353.
- Brook I. Bacteriology of chronic sphenoid sinusitis. Ann Otol Rhinol Laryngol. 2002;111:1002-1004.
- Kovtun AV, Vеngеr LV, Khrаmеnkо NI. Possibility of early diag–nosis of complications of optic neuritis in patients with anterior uveitis according to cogerent tomography of the eye orbit. In: RAD Conference Proceedings. 2020;4:109-12. DOI: 10.21175/RadProc.2020.23. www.rad-proceedings.org (in Ukrainian).
- Venher LV, Kovtun OV, Khramenko NI. Morphometric features of eye structures according to OCT and changes in hemodynamics in patients with anterior uveitis complicated by optic neuritis. Odesa Medical Journal. 2022;1‒2(179‒180):32-38 (in Ukrainian).
- Kovtun OV, Venher LV, Khramenko NI. The nature of the change in hemodynamics of the eye of patients with chronic anterior idiopathic uveitis, the development of neuritis of the visual nerve with its transition to atrophy. Odessa Medical Journal. 2021;5:40-47 (in Ukrainian).
- Venher LV, Kovtun OV, Savko VV. Study of the paranasal sinuses according to computed tomography data in patients with anterior idiopathic uveitis without complications and with the development of neuritis of the visual nerve. Ophthalmol Magazine. 2022;1:37-43 (in Ukrainian).
- Park IH, Song JS, Choi H, Kim TH, Hoon S, Lee SH, Lee HM. Volumetric study in the development of paranasal sinuses by CT imaging in Asian: a pilot study. Int J Pediatr Otorhinolaryngol. 2010 Dec;74(12):1347-50. doi: 10.1016/j.ijporl.2010.08.018. PMID: 20863577.
- Saitakis G, Chwalisz BK. Treatment and Relapse Prevention of Typical and Atypical Optic Neuritis. Int J Mol Sci. 2022 Aug 29;23(17):9769. doi: 10.3390/ijms23179769.
- Храменко Н.І., Величко Л.М., Коновалова Н.В., Богданова О.В., Серебріна Т.М., Журавок Ю.О. Особливості імунологічного статусу та чутливості Т-лімфоцитів периферичної крові до функціональних нейротрансмітерів у хворих на неврит зорового нерва. Офтальмологічний журнал. 2023. № 4(513). С. 14-21.