
Международный неврологический журнал Том 21, №4, 2025
Вернуться к номеру
Синдром вибухового пошкодження. Мігрень присінкового походження
Авторы: S.K. Byelyavsky1, V.I. Lutsenko2, V.M. Pashkovskiy3, K.F. Trinus4, M.A. Trishchynska3, O.Ye. Kononov5
(1) - Kyiv City Clinical Hospital for War Veterans, Kyiv, Ukraine
(2) - Institute of Otolaryngology named after O.S. Kolomiychenko of NAMSU, Kyiv, Ukraine
(3) - Bukovinian State Medical University, Chernivtsi, Ukraine
(4) - Interregional Academy for Staff Management, Kyiv, Ukraine
(5) - Shupyk National Healthcare University of Ukraine, Kyiv, Ukraine
Рубрики: Неврология
Разделы: Клинические исследования
Версия для печати
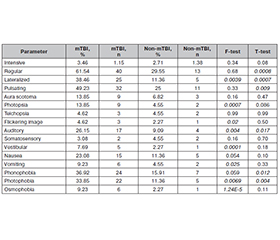
Актуальність. Мігрень є поширеним, багатофакторним, інвалідизуючим, рецидивуючим, спадковим нервово-судинним головним болем. Всесвітня організація охорони здоров’я вважає мігрень найпоширенішим довгостроковим неврологічним станом, який призводить до інвалідизації, враховуючи роки, втрачені через інвалідність. Поширеність мігрені становить 11,7 % (17,1 % у жінок і 5,6 % у чоловіків). Порівняно з попередніми дослідженнями епідеміологічний профіль мігрені залишався стабільним у Сполучених Штатах протягом останніх 15 років. Травма голови викликає кілька тривалих ускладнень, зокрема головний біль. Надзвичайна інтенсивність артилерійських, бомбових, ракетних атак із російської сторони по позиціях українських військових і цивільних містах спонукала нас до вивчення внутрішніх механізмів мігрені, що виникає внаслідок вибухів. Матеріали та методи. Було обстежено 109 хворих: 65 із травматичним ушкодженням мозку легкого (лТУМ) і середнього ступеня без травми голови та 44 без лТУМ (риніт, фарингіт, отит). Опитувальник «Типи запаморочень» використовували відповідно до Міжнародного клінічного протоколу з присінкових розладів (запаморочення). Результати. ЛТУМ при вибуховій травмі супроводжується сильним стресом, об’єктивним і суб’єктивним головокружінням, псевдоголовокружінням та кінетозом, що вважають симптомами ураження присінка, вестибулярного апарату. Запаморочення, ортостатика й агорафобія кількісно значно посилюються при лТУМ, але це не можна вважати специфічним для наслідків вибухової травми. Запаморочення, клаустрофобія та десцендофобія в осіб із лТУМ не мають кількісних змін порівняно з ЛОР-хворими, але є специфічними для лТУМ після вибухової травми. У статистичних дослідженнях важливо використовувати матричний критерій Фішера. Виявилося, що постраждалі із лТУМ мали 3,35 симптому головного болю на людину, тоді як без лТУМ — 1,45. Це означає, що особи із лТУМ мають мігренозний тип болю, а у хворих без лТУМ головний біль немігренозного походження. При вибуховій травмі виникає статистично значущий кількісно та якісно латералізований головний біль зі слуховою аурою та світлобоязню. Такі ознаки зустрічаються у 26,15–38,46 % поранених, що в 6,87 разa більше, ніж у світовій чоловічій популяції. Це означає, що в Україні очікується зростання кількості хворих на мігрень переважно серед чоловічого населення. Крім того, за якісним F-тестом статистично значущими (специфічними для вибухової травми) були скарги на ауру у формі фотопсії, мерехтіння зображень, вестибулярну ауру (запаморочення) з блюванням та осмофобією. Також кількісно значущим виявився регулярний пульсуючий головний біль із фонофобією. Високий рівень кореляції вестибулярних і мігренозних симптомів показав загальні механізми розвитку розладу. Запропоновано гіпотезу про наявність ланцюга подій між лТУМ і нападом мігрені. Вибухова хвиля діє на присінок, природний акселерометр, комплекс отоконіально-волоскових клітин, який механічно представляє масу на живій пружині. Механічна енергія трансформується у зміну електричного потенціалу на мембрані рецептора волоскової клітини, що в подальшому приводить до надмірної генерації потенціалів дії аферентним нейроном та активації вестибулокортикального шляху. Проявом цього є первинна реакція на подію, що травмує: головокружіння, запаморочення, головний біль, нудота, блювання й втрата свідомості. Активація мембранних рецепторів аферентного нейрона приводить до змін у цитоскелеті та концентрації його активних локусів у перинуклеарній зоні, тобто інформація про перезбудження передається від мембранних рецепторів до ядра нейрона. Надалі тривалий час (від днів до років) хворий перебуває в стані уявного благополуччя, проте на рівні присінкових ядер патологічний процес продовжує розвиватися. Поступово в нього втягуються вищі відділи центральної нервової системи, досягаючи кори головного мозку, розгалужуючись на рухові, вегетативні й лімбічні структури. Серед серйозних ускладнень відзначали артеріальну гіпертензію, когнітивні розлади, зниження імунітету. Висновки. Однією з версій патогенезу вестибулярної мігрені є формування больового імпульсу на рівні ядра трійчастого нерва в довгастому мозку через зниження порогу збудливості внаслідок лТУМ.
Background. Migraine is a common, multifactorial, disabling, recurrent, hereditary neurovascular headache disorder. The World Health Organization ranks migraine as the most prevalent, disabling, long-term neurological condition when taking into account years lost due to disability. Prevalence for migraine was 11.7 % (17.1 % in female and 5.6 % in male). Compared with previous studies, the epidemiologic profile of migraine has remained stable in the United States during the past 15 years. Traumatic brain injury causes several long-term disabilities, particularly headaches. Extreme intensity of the artillery, bomb, rocket russian attacks at Ukrainian military positions and civil cities has motivated us to study the intrinsic mechanisms of migraine originating from blast exposure. Materials and methods. One hundred and nine patients were examined: 65 mild traumatic brain injury (mTBI) casualties, who survived mild and moderate blast injury without cranial trauma, and 44 non-mTBI patients (rhinitis, pharyngitis, otitis). Questionnaire “Types of dizziness” has been used according to the International Clinical Protocol on Vestibular Disorders (Dizziness). Results. MTBI from blast injury is accompanied by severe stress, objective and subjective vertigo, giddiness and kinetosis, which are considered to be the symptoms of vestibular damage. Dizziness, orthostatics and agoraphobia are quantitatively significantly increased in mTBI, but it might not be considered specific for blast injury consequences. Giddiness, claustrophobia and descendophobia in mTBI have no quantitative changes compared to the ENT group, but are specific for mTBI after blast injury. It is important to use matrix Fisher test in statistical examinations. It appeared that mTBI casualties have had 3.35 headache symptoms per person, while non-mTBI — 1.45. This fact means that mTBI patients have migraine type of headache and non-mTBI patients have headache of not migraine origin. Blast injury is characterized by statistically significant quantitatively and qualitatively lateralized headache with auditory aura and photophobia. These signs have been met in the range of 26.15–38.46 % of casualties, which is 6.87 times greater than in global male population. It means that in Ukraine we expect an increase in migraine patients mostly in male population. Besides, according to qualitative F-test, complaints of aura photopsia, flickering images, and vestibular aura (giddiness) with vomiting and osmophobia were statistically significant (specific for the blast injury). Also, regular pulsating headache with phonophobia appeared to be quantitatively significant. High-level correlation of vestibular and migraine symptoms has shown the common mechanisms of disorder development. The hypothesis of the event chain between mTBI and migraine attack has been proposed. The blast wave acts on the vestibular natural accelerometer, the otoconia-hair cell complex, which mechanically represents a mass on a living spring. Mechanical energy is transformed into a change in the electrical potential on the membrane of the receptor, hair cell, which further leads to excessive generation of action potentials by the afferent neuron and activation of the vestibulo-cortical pathway. The manifestation of this is the primary reaction to the traumatic event: vertigo, dizziness, headache, nausea, vomiting and loss of consciousness. Activation of membrane receptors of the afferent neuron leads to changes in the cytoskeleton and concentration of its active loci in the perinuclear zone, i.e., information about overexcitation is transmitted from membrane receptors to the nucleus of the neuron. Later, for a long time (from days to years), the patient is in the condition of imaginary well-being, but at the level of the vestibular nuclei, the pathological process continues to develop. Slowly, higher zones of the central nervous system are involved in the pathological process, reaching the cerebral cortex, branching out to motor, vegetative, and limbic structures. Among the serious complications, hypertension, cognitive impairment, and decreased immunity were noted. Conclusions. One of the versions of the vestibular migraine pathogenesis is the formation of a pain impulse at the level of the trigeminal nucleus in the medulla oblongata due to a decrease in the threshold of excitability after mTBI.
легка черепно-мозкова травма; вибухова травма; вестибулярна мігрень
mild traumatic brain injury; blast injury; vestibular migraine