
Журнал «Медицина неотложных состояний» Том 20, №5, 2024
Вернуться к номеру
Періопераційна стратифікація ризиків перед мультирезекційними оперативними втручаннями. Чи достатньо лише класифікації ASA?
Авторы: V.V. Yevsieieva (1), V.I. Cherniy (2), O.I. Plehutsa (1), Yu.B. Lisun (1), S.A. Sheptukha (2)
(1) - State Scientific Institution “Center for Innovative Medical Technologies of the National Academy of Sciences of Ukraine”, Kyiv, Ukraine
(2) - State Scientific Institution “Scientific and Practical Center of Preventive and Clinical Medicine”
of the State Management of Affairs, Kyiv, Ukraine
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
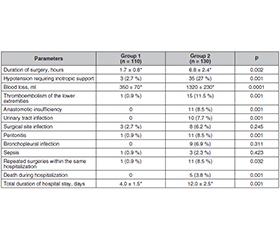
Актуальність. На сьогодні відсутні протоколи лікування хірургічних пацієнтів із коморбідністю. Тому проблема періопераційного ведення хірургічних пацієнтів високого ризику є дуже актуальною, має велике значення для практичної медицини та потребує подальшого вивчення. Одним з найпопулярніших інструментів стратифікації періопераційного ризику залишається шкала Американського товариства анестезіологів (ASA). Мета: оцінити вплив ступеня вираженості хірургічного захворювання й обсягу операції на прогностичну здатність класифікації ASA. Матеріали та методи. До ретроспективного дослідження увійшли 240 пацієнтів із соматичним статусом ASA II, поділені на дві групи залежно від обсягу втручання. Результати. При проведенні кореляційного аналізу встановлено, що тривалість перебування у відділенні інтенсивної терапії, частота повторних надходжень до відділень інтенсивної терапії в межах однієї госпіталізації, смертність, загальна тривалість госпіталізації мають сильний позитивний лінійний зв’язок (r = 0,89, p < 0,001) із обсягом оперативного втручання. Також виявлено сильну позитивну кореляцію між ступенем поширеності системного захворювання та обсягом втручання (r = 0,82, p < 0,001). Спостерігався помірний позитивний зв’язок (r = 0,54, p < 0,001) між тривалістю хірургічної процедури й такими післяопераційними ускладненнями, як тромбоемболія легеневої артерії, неспроможність анастомозу, бронхолегенева інфекція, інфекція сечових шляхів, а також сильний позитивний лінійний зв’язок з інфекцією післяопераційної рани. Висновки. На частоту, характер післяопераційних ускладнень і тривалість госпіталізації вірогідно впливав ступінь тяжкості хірургічної патології та обсяг втручання. Шкала ASA є суб’єктивним інструментом оцінювання летальності й має недостатню прогностичну здатність щодо частоти післяопераційних ускладнень.
Background. As of today, there are no protocols for managing surgical patients with comorbidities. Therefore, the issue of perioperative management of high-risk surgical patients is very relevant, holds significant importance for practical medicine, and requires further study. One of the most popular tools for perioperative risk stratification remains the American Society of Anesthesiologists (ASA) classification. The purpose of the study was to assess the impact of the severity of surgical disease and the extent of surgery on the prognostic ability of the ASA assessment. Materials and methods. The retrospective study included 240 patients with ASA II, divided into 2 groups based on the extent of surgical intervention. Results. Correlation analysis revealed a strong positive linear relationship (r = 0.89, p < 0.001) between the duration of stay in the intensive care unit, the frequency of recurrent admissions to the intensive care unit within the same hospitalization, mortality, the total duration of hospitalization and the extent of surgical intervention. Furthermore, a strong positive correlation (r = 0.82, p < 0.001) was found between the severity of systemic disease spread and the extent of surgical intervention. A moderate positive correlation (r = 0.54, p < 0.001) was observed between the duration of surgical intervention and postoperative complications such as thromboembolism, anastomotic insufficiency, bronchopulmonary, urinary tract infection, as well as a strong positive linear relationship with postoperative wound infection. Conclusions. The frequency, nature of postoperative complications, and duration of hospitalization were significantly influenced by the severity of surgical pathology and the extent of surgical intervention. The ASA classification is a subjective tool for assessing mortality and has inadequate prognostic ability regarding the frequency of postoperative complications.
ASA; передопераційна стратифікація ризиків; покращення якості стратифікації ризиків; пацієнти з високим ризиком періопераційних ускладнень
ASA; preoperative risk stratification; improvement of risk stratification quality; high-risk perioperative complication patients
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Chun-Lin Chu, Hung-Yi Chiou, Wei-Han Chou, Po-Ya Chang, Yi-You Huang, Huei-Ming Yeh. Leading comorbidity associated with 30-day post-anesthetic mortality in geriatric surgical patients in Taiwan: a retrospective study from the health insurance data. BMC Geriatr. 2017 Oct 24;17(1):245. doi: 10.1186/s12877-017-0629-7.
- De Cassai A, Boscolo А, Tonetti Т, Ban I, Ori С. Assignment of ASA-physical status relates to anesthesiologists’ experience: a survey-based national-study. Korean J Anesthesiol. 2019 Feb;72(1):53-59. doi: 10.4097/kja.d.18.00224.
- Shah P, Saran A, Das S. Analysis of the American Society of Anesthesiologists Physical Status Scale Reliability in Anaesthesia Practice: An Observational Study. Turk J Anaesthesiol Reanim. 2020 Oct;48(5):385-390. doi: 10.5152/TJAR.2019.50146.
- Schulz GB, Grimm T, Buchner A, et al. Surgical High-risk Patients With ASA ≥ 3 Undergoing Radical Cystectomy: Morbidity, Mortality, and Predictors for Major Complications in a High-volume Tertiary Center. Clin Genitourin Cancer. 2018 Dec;16(6):e1141-e1149. doi: 10.1016/j.clgc.2018.07.022.
- Normann M, Ekerstad N, Angenete E, Prytz M. Mortality and morbidity after colorectal cancer resection surgery in elderly patients: a retrospective population-based study in Sweden. World J Surg Oncol. 2024 Jan 22;22(1):23. doi: 10.1186/s12957-024-03316-6.
- Hightower CE, Riedel BJ, Feig BW, et al. A pilot study evalua-
- ting predictors of postoperative outcomes after major abdominal surgery: physiological capacity compared with the ASA physical status classification system. Br J Anaesth. 2010 Apr;104:465-471. doi: 10.1093/bja/aeq034.
- Makary MA, Segev DL, Pronovost PJ, et al. Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg. 2010 Jun;210:901-908. doi: 10.1016/j.jamcollsurg.2010.01.028.
- Visnjevac O, Davari-Farid S, Lee J. The Effect of Ad-
- ding Functional Classification to ASA Status for Predicting 30-Day Mortality. Anesth Analg. 2015 Jul;121:110-116. doi: 10.1213/ANE.0000000000000740.
- Jones CR, McCulloch GAJ, Ludbrook G, Babidge WJ, Maddern GJ. Deaths in Incorrectly Identified Low-Surgical-Risk Patients. World J Surg. 2018 Jul;42(7):1997-2000. doi: 10.1007/s00268-017-4427-3.
- ASA Physical Status Classification System. Available from: https://www.asahq.org/standards-and-guidelines/asa-physical-status-classification-system.