
Журнал «Почки» Том 12, №4, 2023
Вернуться к номеру
Показання до нефректомії при захворюваннях нирок: аналіз 10-річного досвіду
Авторы: M.F. Albadran, S.G. Mezban, E.B. Alfadli, K.H. Jareh
Department of Surgery, Urology and Renal Transplantation Center, Al-Sadder Teaching Hospital, Basrah Health Directorate, Ministry of Health, Basrah, Iraq
Рубрики: Нефрология
Разделы: Справочник специалиста, Любимая страница
Версия для печати
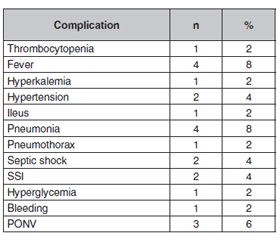
Актуальність. Нефректомія — операція, що виконується в урологічній практиці, — може призвести до необоротного пошкодження нирки під час хірургічного видалення. Мета дослідження: описати 10-річний досвід нефректомії, показання до неї та ускладнення при захворюваннях нирок. Матеріали та методи. Були зібрані дані всіх пацієнтів, які перенесли нефректомію, включаючи демографічні дані, вік, стать, освіту, куріння, споживання алкоголю, етіологію, медичний і хірургічний анамнез та супутню патологію. Показаннями до нефректомії були камені, обструкція, пухлини, пієлонефрит і автосомно-домінантний полікістоз нирок. Серед ускладнень зареєстровані тромбоцитопенія, лихоманка, гіперкаліємія, гіпертензія, кишкова непрохідність, пневмонія, пневмоторакс, септичний шок, інфекція в місці хірургічного втручання, гіперглікемія, кровотеча та післяопераційна нудота й блювання. Передопераційна підготовка включала лабораторні тести, такі як загальний аналіз крові, печінкові та ниркові проби. Доцільно виконати реносцинтиграфію перед нефректомією, щоб розглянути можливість часткового видалення органу. Однак у нашому дослідженні ми проводили її планово, оскільки майже всі пацієнти проходили ультразвукове дослідження або/та комп’ютерну томографію черевної порожнини/таза для виявлення патологій. Черезшкірно вводили поліуретанові катетери або встановлювали стенти. Провідник введено в нирку через жорсткий цистоскоп. Результати. Загалом було виконано 50 нефректомій. Середній вік пацієнтів становив 45 років, коливаючись від 14 до 73 років. Жінок було приблизно 60 %, чоловіків — 40 %. Пацієнти були освіченими (48 %), курили (56 %), споживали алкоголь (12 %), мали обтяжений медичний та хірургічний анамнез (50 %), супутні захворювання (46 %), проживали як у сільській місцевості (44 %), так і у міських районах (56 %). У більшості випадків (52 і 36 %) виявлено відповідно камені або обструкцію. Більшість нефректомій виконано за допомогою лапароскопічного методу (58 %). Відкрите оперативне втручання з приводу спайкового процесу та емфіземи мало місце в 15 випадках (30 %). Ускладнення, пов’язані з лапароскопією та відкритою операцією, виникли в 17 (34 %) пацієнтів. Були зареєстровані тромбоцитопенія, гарячка, гіперкаліємія, гіпертензія, кишкова непрохідність, пневмонія, пневмоторакс, септичний шок, інфекція в місці хірургічного втручання, гіперглікемія, кровотеча та післяопераційна нудота й блювання. Висновки. Кам’яна хвороба та непрохідність були найпоширенішими доброякісними станами, що вимагали нефректомії. За належного досвіду лапароскопічний підхід можна застосовувати при більшості доброякісних захворювань нирок, що потребують нефректомії. Рівень ускладнень при цьому буде порівнянним із таким за відкритої хірургії.
Background. Nephrectomy, a performance surgery in urology practice, may lead to an irreversibly kidney injuries during surgical removal. This study aims to describe 10-years of experience with nephrectomy, its indications and complications in kidney diseases. Materials and methods. Data for all the patients who underwent nephrectomy were collected including demographics, age, sex, education, smoking, alcohol consumption, aetiology, past medical and surgical history and comorbidity. Indications for nephrectomy were stones, obstruction, tumors, pyelonephritis and autosomal dominant polycystic kidney disease. Among complications, thrombocytopenia, fever, hyperkalemia, hypertension, ileus, pneumonia, pneumothorax, septic shock, surgical site infection, hyperglycemia, bleeding and postoperative nausea and vomiting were recorded. Preoperative preparation included laboratory tests such as complete blood count, renal function test and liver function test. It is reasonable to perform renoscintography before nephrectomy to consider partial nephrectomy. However, in our study we performed it routinely because nearly all patients underwent ultrasonography or/and computed tomography scan of abdomen/pelvis to detect pathologies. A percutaneous polyurethane catheters or stents were placed. A guidewire was inserted into the kidney via the rigid cystoscope. Results. A total of 50 nephrectomies were performed. The median age of patients was 45 years ranging from 14 to 73 years. About 60 % of the patients were females and 40 % were males. Patients were educated (48 %), smoking (56 %), alcoholic (12 %), with past medical and surgical history (50 %), comorbidities (46 %) and lived in rural region (44 %) and urban areas (56 %). Stones and obstruction accounted for the majority of cases, 52 and 36 %, respectively. Most of the nephrectomies were performed with laparoscopic approach (58 %). Open surgery was done in 15 cases (30 %) because of adhesions and emphysema. Complications related to laparoscopy and open surgery occurred in 17 (34 %) of patients. Thrombocytopenia, fever, hyperkalemia, hypertension, ileus, pneumonia, pneumothorax, septic shock, surgical site infection, hyperglycemia, bleeding and postoperative nausea and vomiting were recorded. Conclusions. Stone disease and obstruction were the most common benign conditions requiring nephrectomy. The laparoscopic approach can be feasible for most benign kidney diseases requiring nephrectomies with adequate expertise. Сomplication rate in it is comparable with that of open surgery.
нефректомія; хвороби нирок; нефролітіаз; камінь; лапароскопія
nephrectomy; kidney diseases; nephrolithiasis; stone; laparoscopy
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Zelhof B., McIntyre I.G., Fowler S.M., Napier-Hemy R.D., Burke D.M. et al. Nephrectomy for benign disease in the UK: results from the British Association of Urological Surgeons nephrectomy database. BJU Int. 2016. 117. 138-144.
- Breish M.O., Whiting D., Sriprasad S. Laparoscopic Nephrectomy in Patients with Previous Abdominal Surgery. Cureus. 2020 Feb 14. 12(2). e6991. doi: 10.7759/cureus.6991.
- Hadjipavlou M., Khan F., Fowler S., Joyce A., Keeley F.X., Sriprasad S.; BAUS Sections of Endourology and Oncology. Partial vs radical nephrectomy for T1 renal tumours: an analysis from the British Association of Urological Surgeons Nephrectomy Audit. BJU Int. 2016 Jan. 117(1). 62-71.
- El-Asmar J.M., Ayoub C.H., Kfoury P., Abou-Mrad A., El-Hajj A. Surgical Complications Requiring Reoperation in Open Versus Minimally Invasive Radical Nephrectomy: A Contemporary Analysis of the National Surgical Quality Improvement Program. World J. Surg. 2023 Apr. 47(4). 856-862. doi: 10.1007/s00268-022-06869-3.
- Keshavamurthy R., Gupta A., Manohar C.S., KarthikeyanV.S., Singh V.K. Is simple nephrectomy the right nomenclature? Comparing simple and radical nephrectomy to find the answer. J.Family Med. Prim. Care. 2022 Mar. 11(3). 1059-1062.
- Ezomike U.O., Modekwe V.I., Ekenze S.O. Paediatric nephrectomy: patterns, indications and outcome in a developing country. Malawi Med. J. 2018 Jun. 30(2). 94-98. doi: 10.4314/mmj.v30i2.8.
- Demirtaş A., Güleser A.S., Sönmez G., Demirtaş T., TombulŞ.T. Two-step treatment model for the adult patients with an obstructed kidney functioning below 10 % of its capacity: a pilot study. Clin. Exp. Nephrol. 2020 Feb. 24(2). 185-189. doi: 10.1007/s10157-019-01801-x.
- Chiruvella M., Tamhankar A.S., Ghouse S.M., BendigeriM.T., Reddy Kondakindi P.C., Ragoori D. Laparoscopic nephrectomy simplified — a “two-window technique” for safer approach to hilum for a novice. Indian J. Urol. 2018 Oct-Dec. 34(4). 254-259.
- Nasrallah G., Souki F.G. Perianesthetic Management of Laparoscopic Kidney Surgery. Curr. Urol. Rep. 2018 Jan 18. 19(1). 1.
- Jindal T., Mukherjee S., Koju R., Nitesh S., Phom D. Simplifying Laparoscopic Nephrectomy for Beginners: Double Window Technique with En Bloc Hilar Stapling. Cureus. 2021 Jul 1. 13(7). e16090.
- Gächter A., Halling T., Shariat S.F., Moll F.H. Transfer of Knowledge in Urology: A Case Study of Jacob Eduard Polak (1818–1891) and the Introduction of Contemporary Techniques of Lithotomy and Lithotripsy from Vienna to Persia in the Mid-19th Century: A New Analysis of Scientific Papers from the 19th Century. Urol. Int. 2019. 102(1). 1-12. doi: 10.1159/000492156.
- Pang H.Y.M., Chalmers K., Landon B., Elshaug A.G., Matelski J. et al. Utilization Rates of Pancreatectomy, Radical Prostatectomy, and Nephrectomy in New York, Ontario, and New South Wales, 2011 to 2018. JAMA Netw. Open. 2021 Apr 1. 4(4). e215477. doi: 10.1001/jamanetworkopen.2021.5477.
- Khan T.M., Anwar M.S., Shafique Z., Nawaz F.K., KarimM.S. et al. Risk Factors of Nephrolithiasis in a Tertiary Care Hospital in Rawalpindi: A Descriptive Cross-Sectional Study. Cureus. 2022 Jun 24. 14(6). e26274. doi: 10.7759/cureus.26274.
- Clayman R.V., Kavoussi L.R., Soper N.J., Dierks S.M., Meretyk S. et al. Laparoscopic Nephrectomy: Initial Case Report. J. Urol. 2017 Feb. 197(2S). S182-S186. doi: 10.1016/j.juro.2016.10.074.
- Jarzemski P., Listopadzki S., Słupski P., Jarzemski M., Brzoszczyk B. Simultaneous bilateral native nephrectomy by retroperitoneal approach. Int. Braz. J. Urol. 2020 Jul-Aug. 46(4). 538-544. doi: 10.1590/S1677-5538.IBJU.2018.0435.
- Chen Y., Zheng H., Liang G., Wang D., Qiu J., Fang Y. Comparison of Transperitoneal and Retroperitoneal Laparoscopic Nephrectomy for Nonfunctional Tuberculous Kidneys: A Single-Center Experience. J. Laparoendosc. Adv. Surg. Tech. A. 2018 Mar. 28(3). 325-329. doi: 10.1089/lap.2017.0270.
- Wang B., Tian Y., Peng Y., Ban Y., Shan G. et al. Comparative Study of Retroperitoneal Laparoscopic Versus Open Ipsilateral Nephrectomy After Percutaneous Nephrostomy: A Multicenter Analysis. J. Laparoendosc. Adv. Surg. Tech. A. 2020 May. 30(5). 520-524. doi: 10.1089/lap.2019.0746.
- Kurt O., Buldu I., Turan C., Yazici C.M. Does laparoscopic transperitoneal simple nephrectomy for inflammatory and non-inflammatory kidneys differ? Springerplus. 2016 Aug 17. 5(1). 1358. doi: 10.1186/s40064-016-2945-3.
- Gülpınar M.T., Akçay M., Sancak E.B., Akbaş A., TepelerA. et al. Comparison of transperitoneal laparoscopic nephrectomy outcomes in atrophic and hydronephrotic kidneys. Turk. J. Urol. 2015 Dec. 41(4). 181-4. doi: 10.5152/tud.2015.97523.
- Wu G., Wang T., Wang J., Yuan H., Cui Y., Wu J. Complete retroperitoneal laparoscopic nephroureterectomy with bladder cuff excision for upper tract urothelial carcinoma without patient repositioning: a single-center experience. J. Int. Med. Res. 2020 Nov. 48(11). 300060520973915. doi: 10.1177/0300060520973915.
- Li K., Hu C., Huang W., Si-Tu J., Lu L. et al. A modification with threading cannula needle-assisted 4-point suspension fixation for retroperitoneal laparoscopic pyeloplasty in children with ureteropelvic junction obstruction: a cohort study in single center. Int. Urol. Nephrol. 2019 Feb. 51(2). 193-199. doi: 10.1007/s11255-018-2048-x.