
Архив офтальмологии Украины Том 11, №2, 2023
Вернуться к номеру
Аналіз факторів розвитку, клінічного перебігу та особливостей лікування гемофтальму при гіпертонічній ретинопатії
Авторы: Ілюк О.Ю.
Національний медичний університет імені О.О. Богомольця МОЗ України, м. Київ, Україна
Рубрики: Офтальмология
Разделы: Клинические исследования
Версия для печати
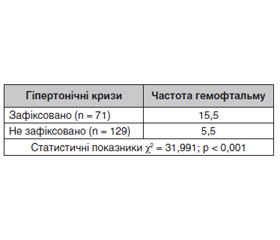
Актуальність. Гіпертонічна хвороба (ГХ) є фактором ризику для розвитку мікросудинних аномалій та оклюзій судин сітківки. Обидва ці патологічні стани можуть бути причиною виникнення крововиливу у склоподібне тіло при гіпертонічній хворобі. Оцінка впливу тяжкості системної патології, стажу захворювання, віку, статі, наявності попередньо визначених офтальмологічних ознак, а також клінічного перебігу та виникнення рецидивів гемофтальму при різних механізмах розвитку є актуальним завданням для сучасної офтальмології. Метою наших досліджень було вивчення особливостей розвитку, клінічного перебігу і хірургічного лікування гемофтальму при гіпертонічній хворобі. Матеріали та методи. Протягом клінічних досліджень обстежено 100 пацієнтів (200 очей), 54 жінки і 46 чоловіків віком від 30 до 82 років, яким було встановлено діагноз гіпертонічної ретинопатії та гемофтальму. Термін динамічного спостереження за пацієнтами з гіпертонічною ретинопатією становив п’ять років. Усі пацієнти дали інформовану добровільну згоду на участь у дослідженні. Згідно з Наказом МОЗ України від 15.03.2007 № 117, усім пацієнтам з гемофтальмом на тлі гіпертонічної ретинопатії спочатку проводилось спостереження та консервативне лікування. При неефективності лікування протягом 4–5 тижнів було виконане хірургічне втручання. Хірургічне втручання проводилось в обсязі закритої субтотальної вітректомії 23/27ga з видаленням внутрішньої обмежувальної мембрани та ендотампонадою газоповітряною сумішшю. Була проаналізована частота виникнення гемофтальму при гіпертонічній ретинопатії з урахуванням статі, віку, стажу загального захворювання, рівня артеріального тиску (АТ), прийому антигіпертензивних препаратів та антикоагулянтів, наявності гіпертонічних кризів в анамнезі, ступеня тяжкості гіпертонічної ретинопатії. Також були оцінені візуальні результати та частота виникнення ускладнень і рецидивів протягом всього терміну спостереження. Результати. Аналіз результатів свідчив, що частота гемофтальму серед пацієнтів з ГХ становила 21 %. Виявлено зростання частоти гемофтальму при ГХ з віком — найбільший рівень спостерігався у віковій групі 61–70 років, з підвищенням рівня АТ, зі збільшенням стажу загального захворювання та за наявності гіпертонічних кризів в анамнезі. Частота гемофтальму була статистично значимо вища за відсутності лікування. Ступінь тяжкості гіпертонічної ретинопатії впливав на частоту виникнення гемофтальму. Встановлено, що 71 % пацієнтів потребували хірургічного лікування. Хірургічне лікування супроводжувалось післяопераційними ускладненнями у 17 % пацієнтів через 2 тижні, у 7 % — через 1 місяць та у 34 % — через 6 місяців після операції. Нами було зафіксовано 7 % рецидивів гемофтальму через 1 місяць після хірургічного лікування та 10 % через 6 місяців. Висновки. Наше дослідження продемонструвало вплив загального стану при гіпертонічній хворобі на клінічній перебіг, виникнення і частоту рецидивів гемофтальму. Хірургічне лікування гемофтальму сприяє статистично значимому поліпшенню зорових функцій та якості життя цієї категорії пацієнтів. Наявність ускладнень і рецидивів після проведеного хірургічного лікування більшою мірою залежить від ступеня тяжкості ГХ у таких пацієнтів.
Background. Hypertension is a risk factor for the development of microvascular anomalies and retinal vessel occlusions. Both pathological conditions can be the cause of hemorrhage in the vitreous body in hypertension. Assessment of the influence of the severity of systemic pathology, disease history, age, gender, the presence of previously diagnosed ophthalmological signs, as well as the clinical course and recurrences of hemophthalmos with various mechanisms of development is an urgent task for modern ophthalmology. The purpose of our research was to study the features of development, clinical course and surgical treatment of hemophthalmos in hypertension. Materials and methods. During clinical studies, 100 patients (200 eyes) were examined: 54 women and 46 men aged 30 to 82 years, who were diagnosed with hypertensive retinopathy and hemophthalmos. Duration of dynamic observation was five years. All patients gave informed voluntary consent to participate in the study. According to the Order of the Ministry of Health of Ukraine No. 117 issued on March, 15, 2007, all patients with hemophthalmos against the background of hypertensive retinopathy were initially observed and conservatively treated. In case of treatment failure for 4–5 weeks, surgical intervention was performed. It was carried out in the scope of a closed subtotal vitrectomy 23/27ga with removal of the inner limiting membrane and endotamponade with a gas-air mixture. The frequency of hemophthalmos in hypertensive retinopathy was analyzed taking into account gender, age, history of the general disease, blood pressure, administration of antihypertensive drugs and anticoagulants, a history of hypertensive crises, the degree of severity of hypertensive retinopathy. Visual results and the frequency of complications and recurrences during the entire observation period were also evaluated. Results. Analysis of the results showed that the frequency of hemophthalmos among patients with hypertension was 21 %. An increase in the frequency of hemophthalmos with hypertension was detected with age — the highest level was observed in the age group of 61–70 years, with an increase in blood pressure, the length of the general illness and with a history of hypertensive crises. The frequency of hemophthalmos was statistically significantly higher in the absence of treatment. The severity of hypertensive retinopathy affected the frequency of hemophthalmos. It was found that 71 % of patients required surgical treatment. Surgical treatment was accompanied by postoperative complications in 17 % of patients after 2 weeks, in 7 % after 1 month, and in 34 %, six months after surgery. We recorded 7% recurrence of hemophthalmos 1 month after surgical treatment and 10% after 6 months. Conclusions. Our study demonstrated the influence of the general condition in hypertension on the clinical course, occurrence and frequency of hemophthalmos recurrences. Surgical treatment of hemophthalmos statistically significant improved visual functions and quality of life in this category of patients. The presence of complications and relapses after surgical treatment largely depends on the severity of hypertension in these patients.
гіпертонічна хвороба; гемофтальм; гіпертонічна ретинопатія; вітректомія
hypertension; hemophthalmos; hypertensive retinopathy; vitrectomy
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Conart J.B., Berrod J.P. Hémorragies du vitré non traumatiques [Non-traumatic vitreous hemorrhage]. J. Fr. Ophtalmol. 2016 Feb. 39(2). 219-25. French. doi: 10.1016/j.jfo.2015.11.001. Epub 2016 Jan 27. PMID: 26826742.
- Shaikh N., Srishti R., Khanum A., Thirumalesh M.B., Dave V., Arora A., et al. Vitreous hemorrhage — Causes, diagnosis, and management. Indian J. Ophthalmol. 2023 Jan. 71(1). 28-38. doi: 10.4103/ijo.IJO_928_22. PMID: 36588205; PMCID: PMC10155538.
- Salcedo-Villanueva G., Trujillo-Alvarez M., Becerra-Revollo C., Ibarra-Elizalde E., Mayorquín-Ruiz M., Velez-Montoya R., et al. A Proposed Method to Quantify Vitreous Hemorrhage by Ultrasound. Clin. Ophthalmol. 2019 Dec 2. 13. 2377-2384. doi: 10.2147/OPTH.S229857. PMID: 31819363; PMCID: PMC6896922.
- Baker M.L., Hand P.J., Wang J.J., Wong T.Y. Retinal signs and stroke — Revisiting the link between the eye and brain. Stroke. 2008. 39. 1371-1379. DOI: 10.1161/ STROKEAHA.107.496091.
- Kitagawa K. Blood pressure management for secondary stroke prevention. Hypertens. Res. 2022 Jun. 45(6). 936-943.
- Chen S., Zeng L., Hu Z. Progressing haemorrhagic stroke: categories, causes, mechanisms and managements. J. Neurol. 2014 Nov. 261(11). 2061-78.
- Ojaghihaghighi S., Vahdati S.S., Mikaeilpour A., Ramouz A. Comparison of neurological clinical manifestation in patients with hemor–rhagic and ischemic stroke. World J. Emerg Med. 2017. 8(1). 34-38.
- An S.J., Kim T.J., Yoon B.W. Epidemiology, Risk Factors, and Clinical Features of Intracerebral Hemorrhage: An Update. 2017. J. Stroke. 2017 Jan. 19(1). 3-10.
- Mechrgui M. Multilayered Hemorrhage Secondary to Retinal Arterial Macroaneurysm Rupture: A Case Report and Review of Literature. Cureus. 2022 Apr 7. 14(4). e23903. doi: 10.7759/cureus.23903. PMID: 35530862; PMCID: PMC9076047.
- Pal B. Retinal arterial macroaneurysm (RAM). eOphtha, Published. April 12, 2021. Available from: https://www.eophtha.com/posts/i-file-retinal-arterial-macroaneurysm-ram. Accessed April 11, 2023.
- Singh D., Tripathy K. Retinal Macroaneurysm. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan–. PMID: 35015432.
- Mirsharif Q., Tajeripour F., Pourreza H. Automated chara–cterization of blood vessels as arteries and veins in retinal images. Computerized Medical Imaging and Graphics. 2013. 37(7–8). 607-617. DOI: 10.1016/j.compmedimag.
- Triantafyllou A., Anyfanti P., Gavriilaki E., Zabulis X., Gka–liag–kousi E., Petidis K., et al. Association Between Retinal Vessel Caliber and Arterial Stiffness in a Population Comprised of Normotensive To Early-Stage Hypertensive Individuals. American Journal of Hypertension. 2014. 27. 1472-1478. DOI: 10.1093/ajh/hpu074.
- Agarwal A.K., Rees C.J., Pollack C.V. Hypertensive Crisis. Cardiology Secrets (Fourth Edition). 2013. 371-379. https://doi.org/10.1016/B978-1-4557-4815-0.00052-0.
- Rapsomaniki E., Timmis A., George J., Pujades-Rodri–guez M., Shah A.D., Denaxas S., et al. Blood pressure and incidence of twelve cardiovascular diseases: Lifetime risks, healthy life-years lost, and age-specific associations in 1·25 million people. Lancet. 383(9932). 1899-1911. https://doi.org/10.1016/S0140-6736(14)60685-1.
- Bhargava M., Ikram M.K., Wong T.Y. How does hypertension affect your eyes? J. Hum. Hypertens. 2012. 26(2). 71-83; Ong Y.-T., Wong T.Y., Klein R., et al. Hypertensive retinopathy and risk of stroke. Hypertension (Dallas, Tex: 1979). 2013. 62(4). 706-11.
- Chen X., Meng Y., Li J., She H.C., Zhao, Zhang J., et al. Serum Uric Acid Concentration Is Associated With Hypertensive Retinophaty In Hypertensive Chinese Adults. BMC Ophthalmology. 2017. 17. 83. DOI: 10.1186/S12886-017-0470-Y.
- Chopra A., Sharma A., Singh S., Bahl V. Changing Perspectives in Classifications of Hypertensive Retinopathy. Journal of Dental and Medical Sciences (IOSR-JDMS). 2014. 13(6). 51-54.
- Unnithan A.K.A., M Das J., Mehta P. Hemorrhagic Stroke. [Updated 2023 May 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559173.
- Singh D., Tripathy K. Retinal Macroaneurysm. [Updated 2023 Feb 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing, 2023 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK576407/.
- Pitkänen L, Tommila P, Kaarniranta K, Jääskeläinen J.E, Kinnunen K. Retinal arterial macroaneurysms. Acta Ophthalmologica. 2014. 92(2). 101-104. https://doi.org/10.1111/aos.12210.
- Hayreh S.S. Retinal vein occlusion. Indian J. Ophthalmol. 1994. 42. 109-32.
- Witmer M.T., Cohen S.M. Oral anticoagulation and the risk of vitreous hemorrhage and retinal tears in eyes with acute posterior vitreous detachment. Retina. 2013. 33(3). 621-626.
- Rossi T., Ripandelli G. Pars Plana Vitrectomy and the Risk of Ocular Hypertension and Glaucoma: Where Are We? J. Clin. Med. 2020 Dec 10. 9(12). 3994. doi: 10.3390/jcm9123994. PMID: 33321697; PMCID: PMC7763583.
- Temkar S., Stephen M., Agarwal D., Kumar Deb А. Multi–layered retinal bleed in ruptured retinal artery macroaneurysm. BMJ Case Reports. 2023. 10.1136/bcr-2023-254669, 16, 4 (e254669).
- Meng Y., Xu Y., Li L., He L., Yi Z., Chen Ch. Retinal arterial macroaneurysm rupture by Valsalva maneuver: a case report and literature review. BMC Ophthalmology. 2022. 10.1186/s12886-022-02662-x, 22, 1.
- Wakabayashi T., Patel N., Bough M., Nahar A., Sheng Y., Momenaei B., et al. Vitrectomy for Vitreous Hemorrhage Associated with Retinal Vein Occlusion: Visual Outcomes, Prognostic Factors, and Sequelae. Retina. 2023 Sep 1. 43(9). 1506-1513. doi: 10.1097/IAE.0000000000003839. PMID: 37294906.
- Dervenis P., Dervenis N., Smith J.M., Steel D.H. Anti-–vascular endothelial growth factors in combination with vitrectomy for complications of proliferative diabetic retinopathy. Cochrane Database Syst. Rev. 2023 May 31. 5(5). CD008214. doi: 10.1002/14651858.CD008214.pub4. PMID: 37260074; PMCID: PMC10230853.