
Журнал «Медицина неотложных состояний» Том 19, №4, 2023
Вернуться к номеру
Капнометрія у відділенні інтенсивної терапії (огляд літератури)
Авторы: Кріштафор Д.А., Кравець О.В., Клигуненко О.М., Єхалов В.В., Станін Д.М.
Дніпровський державний медичний університет, м. Дніпро, Україна
Рубрики: Медицина неотложных состояний
Разделы: Справочник специалиста
Версия для печати
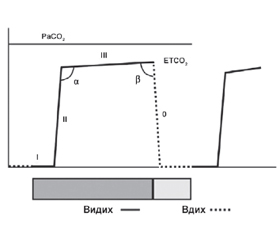
Капнометрія/капнографія — це метод вимірювання та відображення концентрації вуглекислого газу (CO2) у дихальних газах. Найчастіше цей термін передбачає вимірювання парціального тиску вуглекислого газу (PCO2) наприкінці видиху (End-tidal CO2, ETCO2). Крива, що утворюється при капнографії, називається капнограмою, на якій розрізняють інспіраторний та експіраторний сегменти. Основними детермінантами ETCO2 є продукція CO2, серцевий викид, легенева перфузія та альвеолярна вентиляція. У нормі ETCO2 на 2–5 мм рт.ст. нижчий, ніж PCO2 артеріальної крові. Цей градієнт збільшується при порушенні вентиляційно-перфузійних відношень — наприклад, при тромбоемболії легеневої артерії або гіпоперфузії легень під час зупинки кровообігу. Форма капнограми, у свою чергу, залежить від концентрації CO2 в альвеолах та патерну їх спорожнення, а також від серцевого викиду. Це дозволяє використовувати капнографію для реєстрації бронхоспазму, циркуляції CO2 в контурі, спонтанних дихальних спроб тощо. В Україні капнометрія та капнографія рутинно використовуються при анестезіологічному забезпеченні лапароскопічних операцій, які потребують суворого контролю ETCO2 через інсуфляцію CO2 у черевну порожнину та абсорбцію його очеревиною. Разом з тим спектр застосування капнометрії насправді значно ширший, ніж лише лапароскопічна хірургія. У відділенні інтенсивної терапії він включає наступні показання, але не обмежується ними: підтвердження позиції ендотрахеальної трубки при інтубації трахеї; моніторинг цілісності дихального контура, у тому числі при повороті або транспортуванні пацієнта; оцінка ефективності серцево-легеневої реанімації; оцінка ефективності вентиляції маскою; моніторинг дихання під час процедурної седації; моніторинг під час механічної вентиляції легень; допоміжний моніторинг гемодинаміки. У поданому літературному огляді детально розглядаються переваги, недоліки та методика застосування капнометрії/капнографії при кожному з наведених показань.
Capnometry/capnography is a method of measuring and displaying the concentration of carbon dioxide (CO2) in respiratory gases. Most often, this term involves measuring the partial pressure of carbon dioxide (PCO2) at the end of exhalation (end-tidal CO2, ETCO2). The curve formed during capnography is called a capnogram, where the inspiratory and expiratory segments are distinguished. The main determinants of ETCO2 are CO2 production, cardiac output, pulmonary perfusion, and alveolar ventilation. Normally, ETCO2 is 2–5 mm Hg lower than arterial blood PCO2. This gradient increases when the ventilation-perfusion ratio is impaired, for example, in pulmonary embolism or pulmonary hypoperfusion during cardiac arrest. The shape of the capnogram, in turn, depends on the concentration of CO2 in the alveoli and the pattern of their emptying, as well as on cardiac output. This allows the use of capnography to register bronchospasm, CO2 circulation in the circuit, spontaneous breathing attempts, etc. In Ukraine, capnometry and capnography are routinely used in the anesthesia during laparoscopic surgeries, which require strict control of ETCO2 due to the insufflation of CO2 into the abdominal cavity and its absorption by the peritoneum. However, the spectrum of capnometry application is actually much wider than just laparoscopic surgery. In the intensive care unit, it includes but is not limited to the following indications: confirmation of the endotracheal tube position during tracheal intubation; monitoring the respiratory circuit integrity, including while turning and transporting a patient; evaluation of the cardiopulmonary resuscitation effectiveness; evaluation of the mask ventilation effectiveness; breathing monitoring during procedural sedation; monitoring during mechanical ventilation; auxiliary monitoring of hemodynamics. This literature review discusses the advantages, disadvantages and methods of using capnometry/capnography for each of the listed indications in detail.
капнометрія; капнографія; моніторинг; моніторинг у відділенні інтенсивної терапії; вуглекислий газ; огляд
capnometry; capnography; monitoring; monitoring in the intensive care unit; carbon dioxide; review
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Sandroni C., De Santis P., D’Arrigo S. Capnography during cardiac arrest. Resuscitation. 2018. Vol. 132. P. 73-77. doi: 10.1016/j.resuscitation.2018.08.018.
- Walsh B.K., Crotwell D.N., Restrepo R.D. Capnography/Capnometry during mechanical ventilation: 2011. Respir Care. 2011. Vol. 56(4). P. 503-599. doi: 10.4187/respcare.01175.
- Kodali B.S., Urman R.D. Capnography during cardiopulmonary resuscitation: Current evidence and future directions. J. Emerg. Trauma. Shock. 2014. Vol. 7. P. 332-340. doi: 10.4103/0974-2700.142778.
- Kodali B.S. Capnography Outside the Operating Rooms. Anesthesiology. 2013. Vol. 118. P. 192-201. doi: 10.1097/ALN.0b013e318278c8b6.
- Халімончик В.В. Гемодинамічні зміни при лапароскопічних операціях в гінекології. Український медичний часопис. 2019. № 3(131). С. 1-2. doi: 10.32471/umj.1680-3051.131.157727.
- Ткачук О.Л., Парахоняк Р.Л., Мельник С.В., Ткачук-Григорчук О.О. Порівняльна характеристика динаміки кардіоваскулярних та респіраторних ефектів пневмоперитонеуму на основі вуглекислого газу та аргону при лапароскопічній холецистектомії. Art of Medicine. 2021. № 4(20). С. 90-95. DOI: 10.21802/artm.2021.4.20.90.
- Yu T., Cheng Y., Wang X. et al. Gases for establishing pneumoperitoneum during laparoscopic abdominal surgery. Cochrane Database Syst. Rev. 2017. Vol. 6(6). Article No. CD009569. doi: 10.1002/14651858.CD009569.pub3.
- Tan P.L., Lee T.L., Tweed W.A. Carbon dioxide absorption and gas exchange during pelvic laparoscopy. Canadian Journal of Anaesthesia. 1992. Vol. 39(7). P. 677-681. doi: 10.1007/bf03008229.
- Scott D.B., Julian D.G. Observations on cardiac arrhythmias during laparoscopy. BMJ. 1972. Vol. 1. P. 411-413. doi: 10.1136/bmj.1.5797.411.
- Gutt C.N., Oniu T., Mehrabi A. et al. Circulatory and Respiratory Complications of Carbon Dioxide Insufflation. Dig. Surg. 2004. Vol. 21. P. 95-105. doi: 10.1159/000077038.
- Kaloo P., Armstrong S., Kaloo C., Jordan V. Interventions to reduce shoulder pain following gynaecological laparoscopic procedures. Cochrane Database of Systematic Reviews. 2019. Vol. 1(1). Article No. CD011101. DOI: 10.1002/14651858.CD011101.pub2.
- American Society of Anesthesiologists. Standards for Basic Anesthetic Monitoring. Approved by the ASA House of Delegates on October 21, 1986, last amended on October 20, 2010, and reaffirmed on December 13, 2020. URL: https://www.asahq.org/standards-and-guidelines/standards-for-basic-anesthetic-monitoring.
- Adi O., Chuan T.W., Rishya M. A feasibility study on bedside upper airway ultrasonography compared to waveform capnography for verifying endotracheal tube location after intubation. Crit. Ultrasound J. 2013. Vol. 5. P. 7. doi: 10.1186/2036-7902-5-7.
- Quintela P.A., Erroz I.O., Matilla M.M., Blanco S.R., Zubillaga D.M., Santos L.R. Usefulness of bedside ultrasound compared to capnography and X-ray for tracheal intubation. An. Pediatr. 2014. Vol. 81. P. 283-288. doi: 10.1016/j.anpedi.2014.01.004. Spanish.
- Nassar B.S., Schmidt G.A. Capnography During Critical Illness. Chest. 2015. Vol. 149. No. 2. P. 576-585. doi: 10.1378/chest.15-1369.
- Kannan S., Manji M. Survey of use of end-tidal carbon dioxide for confirming tracheal tube placement in intensive care units in the UK. Anaesthesia. 2003. Vol. 58. P. 476-479. doi: 10.1046/j.1365-2044.2002.28934.x.
- Georgiou A.P., Gouldson S., Amphlett A.M. The use of capnography and the availability of airway equipment on Intensive Care Units in the UK and the Republic of Ireland. Anaesthesia. 2010. Vol. 65. P. 462-467. doi: 10.1111/j.1365-2044.2010.06308.x.
- Husain T., Gatward J.J., Hambidge O.R., Asogan M., Southwood T.J. Strategies to prevent airway complications: A survey of adult intensive care units in Australia and New Zealand. Br. J. Anaesth. 2012. Vol. 108. P. 800-806. doi: 10.1093/bja/aes030.
- Soar J., Bottiger B.W., Carli P. et al. European Resuscitation Council Guidelines 2021: Adult advanced life support. Resuscitation. 2021. Vol. 161. P. 115-151. doi: 10.1016/j.resuscitation.2021.02.010.
- Grmec S. Comparison of three different methods to confirm tracheal tube placement in emergency intubation. Intensive Care Med. 2002. Vol. 28. P. 701-704. doi: 10.1007/s00134-002-1290-x.
- Grmec S., Mally S. Prehospital determination of tracheal tube placement in severe head injury. Emergency Medicine. 2004. Vol. 21. P. 518-520.
- Knapp S., Kofler J., Stoiser B. et al. The assessment of four different methods to verify tracheal tube placement in the critical care setting. Anesth. Analg. 1999. Vol. 88. P. 766-770. doi: 10.1097/00000539-199904000-00016.
- Takeda T., Tanigawa K., Tanaka H., Hayashi Y., Goto E., Tanaka K. The assessment of three methods to verify tracheal tube placement in the emergency setting. Resuscitation. 2003. Vol. 56. P. 153-157. doi: 10.1016/s0300-9572(02)00345-3.
- Silvestri S., Ralls G.A., Krauss B. et al. The effectiveness of out-of-hospital use of continuous end-tidal carbon dioxide monitoring on the rate of unrecognized misplaced intubation within a regional emergency medical services system. Ann. Emerg. Med. 2005. Vol. 45(5). P. 497-503. doi: 10.1016/j.annemergmed.2004.09.014.
- Li C.H., Zhao W., Zhang J.H., Jia N.G. Detection of esophageal intubation-assessment of several methods in clinical anesthesia. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2003. Vol. 25(2). P. 197-200. Chinese.
- Anderson D.M. Capnography. Decision Making in Anesthesiology (Fourth Edition). Еd. Bready L.L., Dillman D., Noorily S.H. Mosby, 2007. P. 32-35. doi: 10.1016/B978-0-323-03938-3.50014-2.
- Tanigawa K., Takeda T., Goto E., Tanaka K. Accuracy and reliability of the self-inflating bulb to verify tracheal intubation in out-of-hospital cardiac arrest patients. Anesthesiology. 2000. Vol. 93. P. 1432-1436. doi: 10.1097/00000542-200012000-00015.
- Tanigawa K., Takeda T., Goto E., Tanaka K. The efficacy of esophageal detector devices in verifying tracheal tube placement: a randomized cross-over study of out-of-hospital cardiac arrest patients. Anesth. Analg, 2001. Vol. 92. P. 375-378. doi: 10.1097/00000539-200102000-00018.
- Gandhi S.K., Munshi C.A., Coon R., Bardeen-Henschel A. Capnography for detection of endobronchial migration of an endotracheal tube. J. Clin. Monit. 1991. Vol. 7(1). P. 35-38. doi: 10.1007/BF01617896.
- Ahrens T., Sona C. Capnography application in acute and critical care. AACN Clin. Issues. 2003. Vol. 14(2). P. 123-132. doi: 10.1097/00044067-200305000-00002.
- Cantwell R., Clutton-Brock T., Cooper G. et al. Saving Mo-thers’ Lives: Reviewing maternal deaths to make motherhood safer: 2006–2008. The Eighth Report of the Confidential Enquiries into Maternal Deaths in the United Kingdom. BJOG. 2011. Vol. 118 (Suppl. 1). P. 1-203. doi: 10.1111/j.1471-0528.2010.02847.x.
- Cheifetz I.M., Myers T.R. Respiratory therapies in the critical care setting. Should every mechanically ventilated patient be monitored with capnography from intubation to extubation? Respir. Care. 2007. Vol. 52(4). P. 423-38.
- American Heart Association. 2005 American Heart Association (AHA) guidelines for cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) of pediatric and neonatal patients: pediatric advanced life support. Pediatrics. 2006. Vol. 117(5). P. e1005-e1028. doi: 10.1542/peds.2006-0346.
- Fanara B., Manzon C., Barbot O., Desmettre T., Capellier G. Recommendations for the intra-hospital transport of critically ill patients. Crit. Care. 2010. Vol. 14. P. R87. doi: 10.1186/cc9018.
- Kaneko I. Advanced cardiovascular life support in AHA Guidelines 2010: Key changes from Guidelines 2005. Nihon Rinsho. 2011. Vol. 69(4). P. 623-629. Japanese.
- Lurie K.G., Nemergut E.C., Yannopoulos D., Sweeney M. The physiology of cardiopulmonary resuscitation. Anesth. Analg. 2016. Vol. 122. P. 767-783. doi: 10.1213/ANE.0000000000000926.
- Sanders A.B., Ewy G.A., Taft T.V. Prognostic and therapeutic importance of the aortic diastolic pressure in resuscitation from cardiac arrest. Crit. Care Med. 1984. Vol. 12. P. 871-873. doi: 10.1097/00003246-198410000-00007.
- Niemann J.T., Criley J.M., Rosborough J.P., Niskanen R.A., Alferness C. Predictive indices of successful cardiac resuscitation after prolonged arrest and experimental cardiopulmonary resuscitation. Ann. Emerg. Med. 1985. Vol. 14. P. 521-528. doi: 10.1016/s0196-0644(85)80774-5.
- Paradis N.A., Martin G.B., Rivers E.P. et al. Coronary perfusion pressure and the return of spontaneous circulation in human cardiopulmonary resuscitation. JAMA. 1990. Vol. 263. P. 1106-1113.
- Gudipati C.V., Weil M.H., Bisera J., Deshmukh H.G., Rackow E.C. Expired carbon dioxide: a noninvasive monitor of cardiopulmonary resuscitation. Circulation. 1988. Vol. 77. P. 234-239. doi: 10.1161/01.cir.77.1.234.
- Bhende M.S., Karasic D.G., Karasic R.B. End-tidal carbon dioxide changes during cardiopulmonary resuscitation after experimental asphyxial cardiac arrest. Am. J. Emerg. Med. 1996. Vol. 14(4). P. 349-350. doi: 10.1016/S0735-6757(96)90046-7.
- Paiva E.F., Paxton J.H., O’Neil B.J. The use of end-tidal carbon dioxide (ETCO2) measurement to guide management of cardiac arrest: A systematic review. Resuscitation. 2018. Vol. 123. P. 1-7. doi: 10.1016/j.resuscitation.2017.12.003.
- Kodali B., Urman R. Capnography during cardiopulmonary resuscitation: Current evidence and future directions. J. Emerg. Trauma Shock. 2014. Vol. 7(4). P. 332-340. doi: 10.4103/0974-2700.142778.
- Panchal A.R., Bartos J.A., Cabañas J.G. et al. Adult Basic and Advanced Life Support Writing Group. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020. Vol. 142(16, Suppl. 2). P. S366-S468. doi: 10.1161/CIR.0000000000000916.
- Levine R.L., Wayne M.A., Miller C.C. End-tidal carbon dioxide and outcome of out-of-hospital cardiac arrest. N. Engl. J. Med. 1997. Vol. 337. P. 301-306. doi: 10.1056/NEJM199707313370503.
- Sutton R.M., French B., Meaney P.A. et al. Physiologic monitoring of CPR quality during adult cardiac arrest: A propensity-matched cohort study. Resuscitation. 2016. Vol. 106. P. 76-82. doi: 10.1016/j.resuscitation.2016.06.018.
- Sanders A.B., Kern K.B., Otto C.W., Milander M.M., Ewy G.A. End-tidal carbon dioxide monitoring during cardiopulmonary resuscitation. A prognostic indicator for survival. JAMA. 1989. Vol. 262. P. 1347-1351.
- Garnett A.R., Ornato J.P., Gonzalez E.R., Johnson E.B. End-tidal carbon dioxide monitoring during cardiopulmonary resuscitation. JAMA. 1987. Vol. 257. P. 512-515.
- Pokorna M., Necas E., Kratochvil J., Skripsky R., Andrlik M., Franek O. A sudden increase in partial pressure end-tidal carbon dioxide (P(ET)CO(2)) at the moment of return of spontaneous circulation. J. Emerg. Med. 2010. Vol. 38. P. 614-621. doi: 10.1016/j.jemermed.2009.04.064.
- Lui C., Poon K., Tsui K. Abrupt rise of end tidal carbon dioxide level was a specific but non-sensitive marker of return of spontaneous circulation in patient with out-of-hospital cardiac arrest. Resuscitation. 2016. Vol. 104. P. 53-58. doi: 10.1016/j.resuscitation.2016.04.018.
- Sandroni C., Ristagno G. End-tidal CO2 to detect recovery of spontaneous circulation during cardiopulmonary resuscitation: We are not ready yet. Resuscitation. 2016. Vol. 104. P. 5-6. doi: 10.1016/j.resuscitation.2016.05.018.
- Soar J., Nolan J.P., Böttiger B.W. et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 3. Adult advanced life support. Resuscitation. 2015. Vol. 95. P. 100-147. doi: 10.1016/j.resuscitation.2015.07.016.
- Finer N.N., Rich W., Wang C., Leone T. Airway Obstruction During Mask Ventilation of Very Low Birth Weight Infants During Neonatal Resuscitation. Pediatrics. 2009. Vol. 123. P. 865-869. doi: 10.1542/peds.2008-0560.
- Cereceda-Sánchez F.J., Molina-Mula J. Systematic Review of Capnography with Mask Ventilation during Cardiopulmonary Resuscitation Maneuvers. J. Clin. Med. 2019. Vol. 8(3). P. 358. doi: 10.3390/jcm8030358.
- Hayashida T., Nozaki-Taguchi N., Sato S., Meguro T., Sato Y., Isono S. The use of capnography for real-time monitoring of mask ventilation during induction of general anaesthesia: A prospective observational study. European Journal of Anaesthesiology and Intensive Care. 2022. Vol. 1(6). P. e009. doi: 10.1097/EA9.0000000000000009.
- Chudnofsky C.R., Weber J.E., Stoyanoff P.J. et al. A combination of midazolam and ketamine for procedural sedation and analgesia in adult emergency department patients. Acad. Emerg. Med. 2000. Vol. 7. P. 228-235. doi: 10.1111/j.1553-2712.2000.tb01064.x.
- Sacchetti A., Senula G., Strickland J., Dubin R. Procedural sedation in the community emergency department: Initial results of the ProSCED registry. Acad. Emerg. Med. 2007. Vol. 14. P. 41-46. doi: 10.1197/j.aem.2006.05.023.
- Papachristou G.I., Gleeson F.C., Papachristou D.J., Peter-sen B.T., Baron T.H. Endoscopist administered sedation during ERCP: Impact of chronic narcotic/benzodiazepine use and predictive risk of reversal agent utilization. Am. J. Gastroenterol. 2007. Vol. 102. P. 738-743. doi: 10.1111/j.1572-0241.2007.01093.x.
- Pino R.M. The nature of anesthesia and procedural sedation outside of the operating room. Curr. Opin. Anaesthesiol. 2007. Vol. 20. P. 347-351. doi: 10.1097/ACO.0b013e32827035c7.
- Krauss B., Green S.M. Procedural sedation and analgesia in children. Lancet. 2006. Vol. 367. P. 766-780. doi: 10.1016/S0140-6736(06)68230-5.
- Godwin S.A., Burton J.H., Gerardo C.J. et al. Clinical policy: procedural sedation and analgesia in the emergency department. Ann. Emerg. Med. 2014. Vol. 63(2). P. 247-58. doi: 10.1016/j.annemergmed.2013.10.015.
- Chawla N., Boateng A., Deshpande R. Procedural sedation in the ICU and emergency department. Curr. Opin. Anaesthesiol. 2017. Vol. 30(4). P. 507-512. doi: 10.1097/ACO.0000000000000487.
- Maddox R.R., Oglesby H., Williams C.K., Fields M., Danello S. Continuous Respiratory Monitoring and a “Smart” Infusion System Improve Safety of Patient-Controlled Analgesia in the Postoperative Period. Advances in Patient Safety: New Directions and Alternative Approaches (Vol. 4: Technology and Medication Safety). Еd. by Henriksen K., Battles J.B., Keyes M.A., Grady M.L. Rockville (MD): Agency for Healthcare Research and Quality (US), 2008.
- Krauss B., Hess D.R. Capnography for Procedural Sedation and Analgesia in the Emergency Department. Annals of Emergency Medicine. 2007. Vol. 50. No. 2. P. 172-181. doi: 10.1016/j.annemergmed.2006.10.016.
- Cong M.L., Mohan A. Description of an Assembled Noninvasive Capnography Setup. Air Medical Journal. 2013. Vol. 32. No. 6. P. 343-345. doi: 10.1016/j.amj.2013.08.007.
- McGovern T. Face Mask Capnography. Emergency Medicine Updates. 2015. URL: https://emupdates.com/face-mask-capnography/.
- Hart L.S., Berns S.D., Houck C.S. et al. The value of end-tidal CO2 monitoring when comparing three methods of procedural sedation for children undergoing painful procedures in the emergency department. Pediatr. Emerg. Care. 1997. Vol. 13. P. 189-193. doi: 10.1097/00006565-199706000-00004.
- Miner J.R., Heegaard W., Plummer D. End-tidal carbon dioxide monitoring during procedural sedation. Acad. Emerg. Med. 2002. Vol. 9. P. 275-280. doi: 10.1111/j.1553-2712.2002.tb01318.x.
- Miner J.R., Biros M., Heegaard W. et al. Bispectral EEG analysis of patients undergoing procedural sedation in the emergency department. Acad. Emerg. Med. 2003. Vol. 10. P. 638-643. doi: 10.1111/j.1553-2712.2003.tb00048.x.
- Miner J.R., Biros M., Krieg S. et al. Randomized clinical trial of propofol versus methohexital for procedural sedation during fracture and dislocation reduction in the emergency department. Acad. Emerg. Med. 2003. Vol. 10. P. 931-937. doi: 10.1111/j.1553-2712.2003.tb00646.x.
- Burton J.H., Harrah J.D., Germann C.A. et al. Does end-tidal carbon dioxide monitoring detect respiratory events prior to current sedation monitoring practices? Acad. Emerg. Med. 2006. Vol. 13. P. 500-504. doi: 10.1197/j.aem.2005.12.017.
- Wall B.F., Magee K., Campbell S.G., Zed P.J. Capnography versus standard monitoring for emergency department procedural sedation and analgesia. Cochrane Database Syst. Rev. 2017. Vol. 3(3). Article No. CD010698. doi: 10.1002/14651858.CD010698.pub2.
- Dewdney C., MacDougall M., Blackburn R., Lloyd G., Gray A. Capnography for procedural sedation in the ED: a systematic review. Emerg. Med. J. 2017. Vol. 34(7). P. 476-484. doi: 10.1136/emermed-2015-204944.
- Kartal M., Goksu E., Eray O. et al. The value of ETCO2 measurement for COPD patients in the emergency department. Eur. J. Emerg. Med. 2011. Vol. 8(1). P. 9-12. doi: 10.1097/MEJ.0b013e328337b9b9.
- Delerme S., Freund Y., Renault R. et al. Concordance between capnography and capnia in adults admitted for acute dyspnea in an ED. Am. J. Emerg. Med. 2010. Vol. 28. P. 711-714. doi: 10.1016/j.ajem.2009.04.028.
- Lee S.W., Hong Y.S., Han C. et al. Concordance of end-tidal carbon dioxide and arterial carbon dioxide in severe traumatic brain injury. J. Trauma. 2009. Vol. 67. P. 526-530. doi: 10.1097/TA.0b013e3181866432.
- Rackley C.R. Monitoring During Mechanical Ventilation. Respir. Care. 2020. Vol. 65(6). P. 832-846. doi: 10.4187/respcare.07812.
- Hess D.R., Schlottag A., Levin B. et al. An evaluation of the usefulness of end-tidal PCO2 to aid weaning from mechanical ventilation following cardiac surgery. Respir. Care. 1991. Vol. 36. P. 837-843.
- Tusman G., Suarez-Sipmann F., Bohm S.H., Borges J.B., Hedenstierna G. Capnography reflects ventilation/perfusion distribution in a model of acute lung injury. Acta Anaesthesiol. Scand. 2011. Vol. 55. P. 597-606. doi: 10.1111/j.1399-6576.2011.02404.x.
- Tusman G., Suarez-Sipmann F., Bohm S.H., Pech T., Reismann H., Meschino G. Monitoring dead-space during recruitment and PEEP titration in an experimental model. Intensive Care Med. 2006. Vol. 32. P. 1863-1871. doi: 10.1007/s00134-006-0371-7.
- Böhm S.H., Maisch S., von Sandersleben A. et al. The effects of lung recruitment on the Phase III slope of volumetric capnography in morbidly obese patients. Anesth. Analg. 2009. Vol. 109(1). P. 151-159. doi: 10.1213/ane.0b013e31819bcbb5.
- Tusman G., Groisman I., Fiolo F.E. et al. Noninvasive monitoring of lung recruitment maneuvers in morbidly obese patients: the role of pulse oximetry and volumetric capnography. Anesth. Analg. 2014. Vol. 118(1). P. 137-144. doi: 10.1213/01.ane.0000438350.29240.08.
- Fengmei G., Jin C., Songqiao L., Congshan Y., Yi Y. Dead space fraction changes during PEEP titration following lung recruitment in patients with ARDS. Respir. Care. 2012. Vol. 57(10). P. 1578-1585. doi: 10.4187/respcare.01497.
- Farkas J. Waveform capnography in the intubated patient. The Internet Book of Critical Care. 2021. URL: https://emcrit.org/ibcc/co2/.
- Owen R., Castle N. EtCO2: the key to effective prehospital ventilation. Emerg. Med. J. 2006. Vol. 23(7). P. 578-579. doi: 10.1136/emj.2006.035907.
- Ortega R., Connor C., Kim S., Djang R., Patel K. Monitoring Ventilation with Capnography. N. Engl. J. Med. 2012. Vol. 367. P. e27. doi: 10.1056/NEJMvcm1105237.
- Monnet X., Bataille A., Magalhaes E. et al. End-tidal carbon dioxide is better than arterial pressure for predicting volume responsiveness by the passive leg raising test. Intensive Care Med. 2013. Vol. 39(1). P. 93-100. doi: 10.1007/s00134-012-2693-y.