Резюме
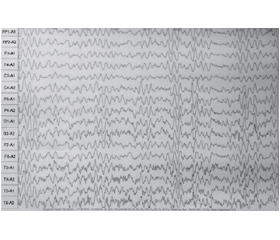
Актуальність. Розвиток та доступність генетичних досліджень як відкривають нові можливості в діагностиці епілептичних енцефалопатій, так і потребують пошуку кореляційних зв’язків між знайденою патологічною мутацією та клініко-інструментальним обстеженням дитини. Зокрема, судомні розлади у дітей, у яких було виявлено SCN1A, охоплюють спектр, що варіює від простих фебрильних судом і генералізованої епілепсії з фебрильними судомами плюс (GEFS+) у легкій формі, що і було вперше описано в 2003 році, до тяжкої міоклонічної епілепсії раннього віку (більш відомої як синдром Драве) чи резистентної дитячої епілепсії з генералізованими тоніко-клонічними нападами (ICE-GTC) у тяжкій формі. Матеріали та методи. Під час дослідження нами було проведено обстеження 4 дітей з клініко-інструментальними ознаками епілептичної енцефалопатії з резистентними нападами, що знаходились на лікуванні у відділенні психоневрології для дітей з перинатальною патологією та орфанними захворюваннями ДУ «Інститут педіатрії, акушерства та гінекології ім. акад. О.М. Лук’янової НАМН України». Середній вік спостережуваних дітей становив 2,2 року (± 1,55). Серед дітей було 2 хлопчиків та 2 дівчаток. Усім дітям, окрім лабораторно-інструментального обстеження, було проведено медико-генетичний аналіз (повногеномне секвенування (WES) або секвенування наступної генерації (NGS)) та виявлено мутацію гена SCN1A. У подальшому з використанням статистичних методів дослідження було проаналізовано взаємозв’язки між отриманими лабораторно-інструментальними та клініко-анамнестичними даними. Результати. Слід відзначити, що дебют генетично детермінованого захворювання, спричиненою SCN1A, припадає на 5,5–6-місячний вік дитини. У дебюті переважають фокальні клонічні, переважно на фоні гіпертермії судоми, які в подальшому модифікуються в генералізовані тоніко-клонічні, міоклонічні і навіть абсанси. У трьох з чотирьох випадків епілептиформна активність мала фокальний характер з переважною локалізацією в лобно-центральних відділах і подальшою генералізацією. У всіх дітей, з огляду на фокальний дебют нападів, початкова терапія проводилася з використанням карбамазепіну, що протипоказано у дітей з цією мутацією. Проаналізувавши наші випадки, ми побачили, що перебіг захворювання та резистентність нападів більш тяжкі у дівчаток. Вивчення цього феномена потребує спостереження за більшою кількістю дітей. Висновки. У дітей з генетично детермінованою епілептичною енцефалопатією, спричиненою мутацією SCN1A, дебют захворювання припадає на перше півріччя життя і проявляється, як правило, фокальними нападами. У дітей із мутацією SCN1A переважає фронтальна локалізація епілептиформної активності. З урахуванням цієї особливості захворювання та на основі власного багаторічного спостереження за дітьми з епілептичними енцефалопатіями раннього віку ми хотіли б застерегти від використання карбамазепінів у цієї вікової групи. Перебіг епілептичної енцефалопатії SCN1A (синдрому Драве) тяжкий, з огляду на резистентність нападів та регрес у розвитку дитини, і часто потребує використання більше ніж 2–3 протиепілептичних препаратів, але правильно підібрана комбінація дозволяє досягти тривалої ремісії.
Background. The development and availability of genetic research open both new possibilities in the diagnosis of epileptic encephalopathies and require the search for correlations between detected pathological mutation and the clinical and instrumental examination of a child. In particular, seizure disorders in children in whom SCN1A has been detected cover a spectrum that varies from simple febrile seizures and mild generalized epilepsy with febrile seizures plus, which was first described in 2003, to severe myoclonic epilepsy in infancy (more commonly known as Dravet syndrome) or severe intractable childhood epilepsy with generalized tonic-clonic seizures. Materials and methods. In our study, we examined 4 children (2 boys and 2 girls) with clinical and instrumental signs of epileptic encephalopathy with resistant seizures who were treated in the psychoneurology department for children with perinatal pathology and orphan diseases of the SI “Lukyanova Institute of Pediatrics, Obstetrics and Gynecology named of the National Academy of Medical Sciences of Ukraine”. The average age of patients was 2.20 ± 1.55 years. In addition to the laboratory and instrumental examination, all children underwent a medical genetic analysis (whole exome sequencing or next-generation sequencing) and the mutation of the SCN1A gene was detected. Subsequently, the relationship between the obtained laboratory instrumental and clinical anamnestic data was analyzed using statistical research methods. Results. It should be noted that the onset of genetic disorders caused by SCN1A occurs at the age of 5.5–6 months. During the onset, focal clonic seizures predominate, mainly against the background of hyperthermia, which are later modified into generalized tonic-clonic, myoclonic ones, and even absences. In three of four cases, the epileptiform activity was focal, with a predominant localization in the fronto-central regions followed by generalization. In all children, taking into account the focal onset of attacks, therapy was started with the use of carbamazepine, which is contraindicated in children with this mutation. After analyzing our cases, we saw that the course of the disease and the resistance of attacks were more severe in girls. The study of this phenomenon requires observation of a larger number of children. Conclusions. In children with genetically determined epileptic encephalopathy caused by the SCN1A mutation, the onset of the disease occurs in the first half of life and is usually manifested itself by focal seizures. In children with SCN1A mutation, frontal localization of epileptiform activity prevails. Considering this feature of the disease and based on our own long-term observation of children with epileptic encephalopathies of early age, we would like to warn against the use of carbamazepines in this age group. The course of SCN1A epileptic encephalopathy (Dravet syndrome) is difficult, given the resistance of attacks and regression in the development of a child, and often requires the use of more than 2–3 antiepileptic drugs, but a correctly selected combination allows long-term remission to be achieved.
Список литературы
1. Кирилова Л., Юзва О., Мірошников О., Бондаренко Н., Берегела О. Генетичні епілептичні та розвиткові енцефалопатії раннього віку: від симптомів до діагнозу. Неонатологія, хірургія та перинатальна медицина. 2023. 13(1(47). 45-52. https://doi.org/10.24061/2413-4260.XIII.1.47.2023.7.
2. Haigh J.L., Adhikari A., Copping N.A. et al. Deletion of a non-canonical regulatory sequence causes loss of Scn1a expression and epileptic phenotypes in mice. Genome Med. 2021. 13. 69. https://doi.org/10.1186/s13073-021-00884-0.
3. Shi X.Y., Tomonoh Y., Wang W.Z., Ishii A., Higurashi N., Kurahashi H., Kaneko S., Hirose S.; Epilepsy Genetic Study Group, Japan. Efficacy of antiepileptic drugs for the treatment of Dravet syndrome with different genotypes. Brain Dev. 2016 Jan. 38(1). 40-6. doi: 10.1016/j.braindev.2015.06.008. Epub 2015 Jul 13. PMID: 26183863.
4. Spampanato J., et al. Generalized epilepsy with febrile seizures plus type 2 mutation W1204R alters voltage-dependet gating of Na(v)1.1 sodium channels. Neuroscience. 2003. 116. 37-48.
5. Miller I.O., Sotero de Menezes M.A. SCN1A Seizure Disorders. 2007 Nov 29 [updated 2022 Feb 17]. In: Adam M.P., Mirzaa G.M., Pagon R.A., Wallace S.E., Bean L.J.H., Gripp K.W., Amemiya A., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2023. PMID: 20301494.
6. Ding J., Li X., Tian H., Wang L., et al. SCN1A Mutation-Beyond Dravet Syndrome: A Systematic Review and Narrative Synthesis. Front Neurol. 2021. 12. 743726. doi: 10.3389/fneur.2021.743726.
7. Chen C., Fang F., Wang X., Lv J., Wang X., Jin H. Phenotypic and Genotypic Characteristics of SCN1A Associated Seizure Diseases. Front. Mol. Neurosci. 2022. 15. 821012. doi: 10.3389/fnmol.2022.821012.
8. Wirrell E.C., Laux L., Donner E., et al. Optimizing the Diagnosis and Management of Dravet Syndrome: Recommendations From a North American Consensus Panel. Pediatr. Neurol. 2017. 68. 18-34.e3. doi: 10.1016/j.pediatrneurol.2017.01.025.
9. Rilstone J.J., Coelho F.M., Minassian B.A., Andrade D.M. Dravet syndrome: seizure control and gait in adults with different SCN1A mutations. Epilepsia. 2012. 53(8). 1421-8. doi: 10.1111/j.1528-1167.2012.03583.x.
10. Aljaafari D., Fasano A., Nascimento F.A., et al. Adult motor phenotype differentiates Dravet syndrome from Lennox-Gastaut syndrome and links SCN1A to early onset parkinsonian features. Epilepsia. 2017. 58(3). e44-e48. doi: 10.1111/epi.13692.
11. Bayat A., Hjalgrim H., Møller R.S. The incidence of SCN1A-related Dravet syndrome in Denmark is 1:22,000: a population-based study from 2004 to 2009. Epilepsia. 2015. 56(4). e36-9. doi: 10.1111/epi.12927.
12. Wu Y.W., Sullivan J., McDaniel S.S., et al. Incidence of Dravet Syndrome in a US Population. Pediatrics. 2015. 136(5). e1310-5. doi: 10.1542/peds.2015-1807.
13. Cornejo-Sanchez D.M., Acharya A., Bharadwaj T., Marin-Gomez L., et al. SCN1A Variants as the Underlying Cause of Genetic Epilepsy with Febrile Seizures Plus in Two Multi-Generational Colombian Families. Genes (Basel). 2022. 13(5). 754. doi: 10.3390/genes13050754.
14. Brunklaus A., Ellis R., Reavey E., Forbes G.H., Zuberi S.M. Prognostic, clinical and demographic features in SCN1A mutation-positive Dravet syndrome. Brain. 2012. 135(Pt 8). 2329-36. doi: 10.1093/brain/aws151.
15. Ragona F., Granata T., Dalla Bernardina B., et al. Cognitive development in Dravet syndrome: a retrospective, multicenter study of 26 patients. Epilepsia. 2011. 52(2). 386-92. doi: 10.1111/j.1528-1167.2010.02925.x.
16. de Lange I.M., Gunning B., Sonsma A.C.M., et al. Influence of contraindicated medication use on cognitive outcome in Dravet syndrome and age at first afebrile seizure as a clinical predictor in SCN1A-related seizure phenotypes. Epilepsia. 2018. 59. 6. 1154-1165. https://doi.org/10.1111/epi.14191.
17. Scheffer I.E., Nabbout R. SCN1A-related phenotypes: Epilepsy and beyond. Epilepsia. 2020. 60. 3. 17-24. https:// doi.org/10.1111/epi.16386.
18. Sullo F., Pasquetti E., Patanè F. et al. SCN1A and Its Related Epileptic Phenotypes. Journal of Pediatric Neurology. 2023. 21(03). 155-167. DOI: 10.1055/s-0041-1727260.
19. Wirrell E.C., Hood V., Knupp K.G., et al. International consensus on diagnosis and management of Dravet syndrome. Epilepsia. 2022. 63(7). 1761-1777. doi: 10.1111/epi.17274.
20. Wilmshurst J.M., Gaillard W.D., Vinayan K.P., et al. Summary of recommendations for the management of infantile seizures: Task Force Report for the ILAE Commission of Pediatrics. Epilepsia. 2015. 56(8). 1185-97. doi: 10.1111/epi.13057.
21. Rodda J.M., Scheffer I.E., McMahon J.M., Berkovic S.F., Graham H.K. Progressive gait deterioration in adolescents with Dravet syndrome. Arch. Neurol. 2012. 69(7). 873-8. doi: 10.1001/archneurol.2011.3275.
22. Fukuma G., Oguni H., Shirasaka Y., et al. Mutations of neuronal voltage-gated Na+ channel alpha 1 subunit gene SCN1A in core severe myoclonic epilepsy in infancy (SMEI) and in borderline SMEI (SMEB). Epilepsia. 2004. 45(2). 140-8. doi: 10.1111/j.0013-9580.2004.15103.x.
23. Brunklaus A., Brünger T., Feng T., et al. The gain of function SCN1A disorder spectrum: novel epilepsy phenotypes and therapeutic implications. Brain. 2022. 145(11). 3816-3831. doi: 10.1093/brain/awac210.
24. Dutton S.B.B., Dutt K., Papale L.A., et al. Early-life febrile seizures worsen adult phenotypes in Scn1a mutants. Exp. Neurol. 2017. 293. 159-171. doi: 10.1016/j.expneurol.2017.03.026.
25. Hattori J., Ouchida M., Ono J., Miyake S., et al. A screening test for the prediction of Dravet syndrome before one year of age. Epilepsia. 2008. 49(4). 626-33. doi: 10.1111/j.1528-1167.2007.01475.x.
26. Verbeek N.E., van Kempen M., Gunning W.B., et al. Adults with a history of possible Dravet syndrome: an illustration of the importance of analysis of the SCN1A gene. Epilepsia. 2011. 52(4). e23-5. doi: 10.1111/j.1528-1167.2011.02982.x.
27. Harkin L.A., McMahon J.M., Iona X., Dibbens L., et al. The spectrum of SCN1A-related infantile epileptic encephalopathies. Brain. 2007. 130(Pt 3). 843-52. doi: 10.1093/brain/awm002.
28. Ok Kim Y., Bellows S., McMahon Ja.M. et al. Atypical multifocal Dravet syndrome lacks generalized seizures and may show later cognitive decline. Dev. Med. & Child Neurology. 2014. 56. 1. 85-90. https://doi.org/10.1111/dmcn.12322.
29. Helbig I., Goldberg E. The dose makes the poison-Novel insights into Dravet syndrome and SCN1A regulation through nonproductive splicing. PLoS Genet. 2021. 17(1). e1009214. doi: 10.1371/journal.pgen.1009214.
30. Sadleir L.G., Mountier E.I., Gill D., et al. Not all SCN1A epileptic encephalopathies are Dravet syndrome Early profound Thr226Met phenotype. Neurology. 2017. 89 (10). 1035042. DOI: 10.1212/WNL.0000000000004331.
31. Gowda V.K., Amoghimath R., Battina M., Shivappa S.K., Benakappa N. Case Series of Early SCN1A-Related Developmental and Epileptic Encephalopathies. J. Pediatr. Neurosci. 2021. 16(3). 212-217. doi: 10.4103/jpn.JPN_99_20.
32. McIntosh A.M., McMahon J., Dibbens L.M., Iona X., Mulley J.C., Scheffer I.E., Berkovic S.F. Effects of vaccination on onset and outcome of Dravet syndrome: a retrospective study. Lancet Neurol. 2010. 9 (6). 592-8. doi: 10.1016/S1474-4422(10)70107-1.
33. Tro-Baumann B., von Spiczak S., Lotte J., Bast T. et al. A retrospective study of the relation between vaccination and occurrence of seizures in Dravet syndrome. Epilepsia. 2011. 52(1). 175-8. doi: 10.1111/j.1528-1167.2010.02885.x.
34. Wong P.T., Wong V.C. Prevalence and Characteristics of Vaccination Triggered Seizures in Dravet Syndrome in Hong Kong: A Retrospective Study. Pediatr. Neurol. 2016. 58. 41-7. doi: 10.1016/j.pediatrneurol.2016.01.011.
35. Tsuji M., Mazaki E., Ogiwara I., et al. Acute encephalopathy in a patient with Dravet syndrome. Neuropediatrics. 2011. 42(2). 78-81. doi: 10.1055/s-0031-1279725. Epub 2011 Jun 6. PMID: 21647847.
36. Isom L.L. Is Targeting of Compensatory Ion Channel Gene Expression a Viable Therapeutic Strategy for Dravet Syndrome? Epilepsy Curr. 2019. 19(3). 193-195. doi: 10.1177/1535759719844780.
37. Wirrell E.C., Laux L., Franz D.N., Sullivan J. Stiripentol in Dravet syndrome: results of a retrospective U.S. study. Epilepsia. 2013. 54(9). 1595-604. doi: 10.1111/epi.12303.
38. Inoue Y., Ohtsuka Y. STP-1 Study Group. Long-term safety and efficacy of stiripentol for the treatment of Dravet syndrome: A multicenter, open-label study in Japan. Epilepsy Res. 2015. 113. 90-7. doi: 10.1016/j.eplepsyres.2015.03.012.
39. Devinsky O., Cross J.H., Laux L., Marsh E., Miller I., Nabbout R., Scheffer I.E., Thiele E.A., Wright S.; Cannabidiol in Dravet Syndrome Study Group. Trial of Cannabidiol for Drug-Resistant Seizures in the Dravet Syndrome. N. Engl. J. Med. 2017 May 25. 376(21). 2011-2020. doi: 10.1056/NEJMoa1611618.
40. Ceulemans B., Schoonjans A.S., Marchau F., Paelinck B.P., Lagae L. Five-year extended follow-up status of 10 patients with Dravet syndrome treated with fenfluramine. Epilepsia. 2016. 57(7). e129-34. doi: 10.1111/epi.13407.
41. Strzelczyk A., Schubert-Bast S. A Practical Guide to the Treatment of Dravet Syndrome with Anti-Seizure Medication. CNS Drugs. 2022 Mar. 36(3). 217-237. doi: 10.1007/s40263-022-00898-1.
42. Tian X., Chen J., Zhang J., Yang X., Ji T., Zhang Y., Wu Y., Fang F., Wu X. Zhang Y. The Efficacy of Ketogenic Diet in 60 Chinese Patients with Dravet Syndrome. Front. Neurol. 2019. 10. 625. doi: 10.3389/fneur.2019.00625.
43. Steel D., Symonds J.D., Zuberi S.M., Brunklaus A. Dravet syndrome and its mimics: Beyond SCN1A. Epilepsia. 2017 Nov. 58(11). 1807-1816. doi: 10.1111/epi.13889. Epub 2017 Sep 7. PMID: 28880996.