Unilateral neglect (or hemineglect) is a neuropsychological syndrome, the feature of which is the loss of the ability to respond to contralesional stimuli, despite intact sensory or motor nerve pathways [1–4]. In other words, visuospatial neglect of the opposite side of the focus develops, as well as ignoring and not realizing the motor deficit [5].
The causes for the development of the neglect pheno-menon might be: cerebral infarction, traumatic brain injury, space-occupying lesion and brain surgery [2].
The most common cause of this syndrome is a stroke in the subdominant hemisphere (right) [6]. Hemineglect in the lesion of the left hemisphere is much less common [7–9] because it is the right hemisphere that plays a key role in the processes of attention [10]. The lack of compensation for right-sided damage is explained by the fact that the left hemisphere perceives only the opposite side of space, while the right hemisphere perceives both sides [11].
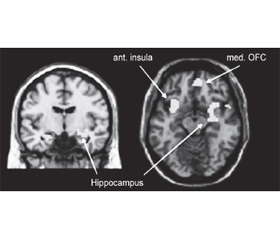
It is believed that a certain concentration and distribution of neurotransmitters regulate attention. This distribution is uneven in different hemispheres of the brain. The norepinephrine mediator system produces norepinephrine and serotonin, which are especially important for the processes of excitation and scanning the environment. This system is lateralized to the right hemisphere. The part of the thalamus that connects to the right hemisphere has a higher concentration of norepinephrine than the part that connects to the left hemisphere (Fig. 1). This asymmetry can be traced in the area of the cerebral cortex. Pathological processes in the structure of the right hemisphere damage to the norepinephrine mediator system. This damage reduces sensitivity and the ability to respond quickly to new environmental stimuli [10, 12].
There are several approaches to the classification of hemineglect syndrome. The unilateral neglect can be classified as egocentric or allocentric ignoring [14]. This classification is built based on the perception of spatial landmarks [10]. For a long time, it was considered that neuroanatomically and pathogenetically these two processes are completely different [15]. However, over time, it turned out that these different behavioral disorders have a single pathogenetic mechanism [16].
In egocentric hemineglect, the midline is determined from the central axis of the patient’s neck, torso, and retina (spectator-oriented), whereas in allocentric hemineglect, the midline is determined from the central axis of the stimulus, regardless of its position in the environment (stimulus-oriented). In the vast majority of patients with the phenomenon of ignoring, egocentric hemineglect is observed [14, 17]. In other words, a person with the lesion of the right hemisphere of the brain in egocentric neglect loses the ability to respond to information coming from the left side of the body, and in allocentric — the ability to respond to the left side of each object, regardless of the position of this object to the patient (Fig. 2). In some patients, both of these variants with diffe-rent degrees of manifestation may be observed [10].
/43.jpg)
The neglect syndrome can also be classified into sensory, motor and representative. Sensory, in turn, can be visual, defined as the inability to detect stimuli present in the contra-lesional visual field, or auditory, which is determined by lack of attention to sounds or verbal stimuli from the contralateral space. Motor hemineglect is the inability to spontaneously use the limb but without primary motor or sensory deficit. A representative variant is most often determined by the manifestations of autometamorphopsia [18, 19].
Unilateral neglect is a heterogeneous syndrome with a large number of variations of symptoms. Patients perceive and process information on the “non-electronic” side, sometimes demonstrate a rather complex reaction to it but do not realize it. During daily activities, they can eat only on the ipsilesional side of the plate, come across objects on the contralesional side while walking, skip the beginning of sentences while reading, do not dress on the contralesional side of the body, and wash, shave or apply cosmetics only on the ipsilesional side of the face or body [20]. Also, one of the manifestations of unilateral neglect is the deviation of the head and gaze towards the lesion, which occurs involuntarily but without signs of gaze palsy [19].
At the end of the 20th century, a new scientific discipline emerged, which was called neuroaesthetics. The term was suggested by the British professor of neurobiology Semir Zeki. Prior to that, it was a part of cognitive science, neurobiology and aesthetics [21]. The development of neuroaesthetics was greatly influenced by the work of Indian neurologist Vilayanur Ramachandran who is known around the world for his study of mirror neurons. It was he who proposed the nine laws of neuroaesthetics that remain relevant today. Neuroaesthetics generally refers to the study of the neural foundations of beauty by understanding the mechanisms underlying the brain’s response to art. The main purpose is to determine the nerve correlates associated with aesthetic experiences [26]. There are more and more new researches and discoveries every year, which undoubtedly indicate the relevance of this issue and its further potential [21]. Nowadays, neuroaesthetics is not limited to the accumulation of knowledge only through the prism of art but includes a large number of scientific works, the practical significance of which is the use of its achievements in many fields, including health care.
It is proved that the feeling of beauty is natural, as it is provided by universal innate mechanisms of visual sensation. Since this process is not acquired, it occurs by default, regardless of the person’s wishes. Therefore, depending on the situation, interpretations and judgments that arise in the brain as a result of perception can be a source of pleasure and relieve stress or, conversely, suppress and cause discomfort [22, 23].
If we are based on the doctrine of neuroaesthetics, then some of its laws can explain the mechanisms of development of unilateral neglect. So, one of them is the law of attraction to symmetry. Evolutionarily, the entire organism is built on the principle of bilateral symmetry, and asymmetry is associated with infection and disease [24], so it is less attractive for perception by our nervous system. Hence our innate desire to prefer something proportional and symmetrical. After a vascular catastrophe, a unilateral neurological deficit develops in the cerebral hemisphere, which provokes asymmetry of the whole body and its functions. Therefore, it is natural that the nervous system tries to alleviate stress and ignore this situation.
Under conditions of oxidative stress, in which the brain is after a stroke, it becomes much more difficult to provide the basic primary properties of attention (stability, volume, distribution, selectivity and concentration) [25]. In this case, another law of neuroaesthetics is connected — isolation of one module and distribution of attention [24]. The subconscious, which is already trying to ignore the asymmetric neurological deficit, begins to focus on the healthy side and allocate it as the main module of perception.
The pathological circle of unilateral neglect from the standpoint of neuroaesthetics is fixed by the principle of peak displacement. In other words, the signal gains in the selected modality. As a result of redistribution and concentration of attention on one healthy side, hyperbolized perception of stimuli by sensory systems develops, and this leads to greater aesthetic pleasure than from stimuli under normal conditions. Vilayanur Ramachandran called this process of exaggerated perception a “superstimulus”.
However, there is a great deal of heterogeneity in neuroscientific researches on neurological correlates related to aesthetic experiences (eg, evaluation and perception of attractive stimuli). This discrepancy is usually explained by the lack of consensus on the definition of “aesthetic experience”. Usually, trying to understand the biological and neural basis of aesthetic experience, to explain how aesthetic experiences are created in the brain, and to use our know-ledge of brain mechanisms to inform our understanding of these experiences is certainly a necessary step. In this sense, the contribution of neuroaesthetics is crucial in shaping the understanding of aesthetic experience. However, the precondition for this is that neuroaesthetics becomes more critical and contextualized [26, 27].
Summarizing all the above, unilateral neglect (or hemineglect) is a complex heterogeneous neuropsychological syndrome, the final pathogenetic mechanism of which is not fully understood and has a large basis for further researches. Using some laws and principles of the modern discipline of neuroaesthetics, we can use neurobiological and psychological processes of the brain’s perception of beauty to try to explain the “interest” of consciousness in unilateral neglect.
The laws of peak displacement (or “superstimulus”), isolation, symmetry of neuroaesthetics make it possible to understand the biological and neural basis of the brain mechanisms of hemineglect syndrome, as well as their role in reducing shock to the patient’s mind under oxidative stress.
Further researches contextualized in this direction will significantly increase the effectiveness of rehabilitation of patients who have suffered from a brain infarction, the level of their social and household adaptation and, accordingly, the quality of life.
Conflict of interest. The authors declare the absence of a conflict of interest in the preparation of this article.
Received 22.03.2021
Revised 02.04.2021
Accepted 09.04.2021
Список литературы
1. Jordan E. Pierce, Roberta Ronchi, Marine Thomasson, Irene Rossi, Carlotta Casati, Arnaud Saj, Giuseppe Vallar, Patrik Vuilleumier. A novel computerized assessment of manual spatial exploration in unilateral spatial neglect. Neuropsychological Rehabilitation. 2021. doi: 10.1080/09602011.2021.1875850.
2. DeDios-Stern S., Durkin N.M., Soble J.R. Case of right hemispatial neglect and transcortical sensory aphasia following left occipitotemporoparietal glioblastoma resection. 2019. doi: 10.1080/23279095.2019.1590357.
3. Rossit S. Action and rehabilitation in hemispatial neglect. 2019. http://theses.gla.ac.uk/820.
4. Lunven M., Bartolomeo P. Attention and spatial cognition: neural and anatomical substrates of visual neglect. Ann. Phys. Rehabil. Med. 2017. 60(3). 124-129. doi: 10.1016/j.rehab.2016.01.004.
5. Дідо Ю., Дуло О. Особливості порушення функцій в осіб із правопівкульним ішемічним інсультом, ускладненим неглектом із позиції фізичного терапевта. Молодіжний науковий вісник Східноєвропейського національного університету імені Лесі Українки. 2018. 32. 78-85.
6. Kerkhoff G., Rode G., Clarke S. Treating neurovisual deficits and spatial neglect. In: Platz T. (eds) Clinical pathways in stroke rehabilitation. Cham: Springer; 2021. doi: 10.1007/978-3-030-58505-1_11.
7. Heilman K.M., Abell T.V.D. Right hemisphere dominance for attention: the mechanism underlying hemispheric asymmetries of inattention (neglect). Neurology. 1980. 30. 327-330. doi: 10.1212/wnl.30.3.327.
8. Галкин А.С. и др. Возможности повышения эффективности реабилитации пациентов после инсульта с синдромом игнорирования. Журнал неврологии и психиатрии им. С.С. Корсакова. 2014. 10. 30-34.
9. Ковальчук В.В., Шварцман Г.И., Гусев А.О. Причины необходимости и способы устранения синдромов неглекта и «отталкивания» у пациентов после инсульта — факторов, препятствующих проведению адекватной реабилитации. Медико-социальная экспертиза и реабилитация. 2013. 2. 50-53.
10. Laksmidewi Anak Agung Ayu Putri, Putu Lohita Rahmawati. Spatial frames of visual hemineglect in patient with high-grade glioma: a case report and review of literature. International Journal of Medical Reviews and Case Reports. 2020. 4(11). 95-99. doi: 10.5455/IJMRCR.high-grade-glioma-visual.
11. Насонова Т.І. та ін. Синдром ніглекту після ішемічного інсульту: діагностика, можливості лікування. Український вісник психоневрології. 2019. 27, 2(99). 8-14.
12. Bowen A., McKenna K., Tallis R.C. Reasons for variability in the reported rate of occurrence of unilateral spatial neglect after stroke. Stroke. 1999. 30. 1196-1202. doi: 10.1161/01.str.30.6.1196.
13. Ding Y.S. Progress in PET imaging of the norepinephrine transporter system. In: Dierckx R.A., Otte A., de Vries E.F., van Waarde A., Lammertsma A.A. (eds). PET and SPECT of neurobiological systems. Cham: Springer, 2021. doi: 10.1007/978-3-030-53176-8_20.
14. Ishii D., Osaki H., Yozu A., Ishibashi K., Kawamura K., Yamamoto S., Miyata M., Kohno Y. Ipsilesional spatial bias after a focal cerebral infarction in the medial agranular cortex: a mouse model of unilateral spatial neglect. Behav. Brain Res. 2021 Mar 5. 401. 113097. doi: 10.1016/j.bbr.2020.113097. Epub 2020 Dec 29. PMID: 33385423.
15. Karnath H., Ferber S., Kimmelbach M. Spatial awareness is a function of the temporal not the posterior parietal lobe. Nature. 2001. 411. 950-3. doi: 10.1038/35082075.
16. Rorden C. et al. Allocentric neglect strongly associated with egocentric neglect. Neuropsychologia. 2012. 50(6). 1151-1157. doi: 10.1016/j.neuropsychologia.2012.03.031.
17. Kortte Kathleen, Hillis Argye. Recent advances in the understanding of neglect and anosognosia following right hemisphere stroke. Current Neurology and Neuroscience Reports. 2009. 9. 459-65. doi: 10.1007/s11910-009-0068-8.
18. Spaccavento S., Cellamare F., Falcone R., Loverre A., Nardulli R. Effect of subtypes of neglect on functional outcome in stroke patients. Ann. Phys. Rehabil. Med. 2017 Nov. 60(6). 376-381. doi: 10.1016/j.rehab.2017.07.245.
19. Rode G., Pagliari C., Huchon L., Rossetti Y., Pisella L. Semiology of neglect: an update. Annals of Physical and Rehabilitation Medicine. 2017. 60(3). 177-185. doi: 10.1016/j.rehab.2016.03.003.
20. Gammeri R., Iacono C., Ricci R., Salatino A. Unilateral spatial neglect after stroke: current insights. Neuropsychiatr. Dis. Treat. 2020. 16. 131-152. doi: 10.2147/NDT.S171461.
21. Оболенська М. Філософія нейроестетики в музичному мистецтві. Вісник Харківського національного університету імені В.Н. Каразіна. Серія «Теорія культури і філософія науки». 2019. 60. 80-89. https://periodicals.karazin.ua/thcphs/article/view/14108.
22. Zeki S. Inner vision: an exploration of art and the brain. 2002.
23. Nanda U., Pati D., McCurry K. Neuroesthetics and healthcare design. HERD: Health Environments Research & Design Journal. 2009. 2(2). 116-133. doi: 10.1177/193758670900200210.
24. Ramachandran Vilayanur, William Hirstein. The science of art: а neurological theory of aesthetic experience. Journal of Сonsciousness Studies. 1999. 6(6–7). 15-51.
25. Федченко Т.Л. Рівень сформованості уваги та уважності учнів початкових класів спеціального закладу середньої освіти для дітей з порушенням розумового розвитку. Кваліфікаційна робота (проєкт) на здобуття ступеня вищої освіти “магістр”, 2020.
26. Koukouti M.D., Malafouris L. Thinging beauty: anthropological reflections on the making of beauty and the beauty of making. Reti, Saperi, Linguaggi. 2020. 9(18). 211-238.
27. Gallese V. Brain, body, habit and the performative quality of aesthetics. In: Testa I., Caurana F. (eds). Habits: pragmatist appro-aches from cognitive neuroscience to social science. Cambridge, UK: Cambridge University Press, 2021, in press. PsyArXiv, 1 June 2020. doi: 10.31234/osf.io/sge5m.

/43.jpg)