
Журнал «Травма» Том 26, №5, 2025
Вернуться к номеру
Клініко-анатомічна структура дефектів довгих кісток у віковому аспекті
Авторы: Гур’єв С.О. (1), Кушнір В.А. (1), Гаріян С.В. (2), Цибульський О.С. (2)
(1) - Державний заклад «Український науково-практичний центр екстреної медичної допомоги та медицини катастроф МОЗ України», м. Київ, Україна
(2) - Тернопільська обласна клінічна лікарня, м. Тернопіль, Україна
Рубрики: Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
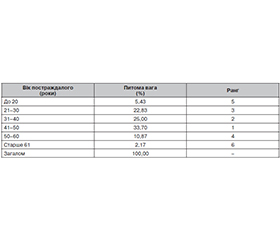
Актуальність. Дефекти довгих кісток (ДДК) є зазвичай наслідком високоенергетичної травми та мають тенденцію до поширення у постраждалих. Така патологія не тільки потребує довготривалого лікування, а й призводить до високого ризику інвалідизації постраждалого внаслідок як самого дефекту, так і можливої ампутації кінцівки. Матеріали та методи. Дослідження має когортний характер і базоване на вивченні й аналізі 92 випадків ДДК кінцівок, що виникли внаслідок бойових уражень під час воєнних дій на території України у період із 2022 по 2024 рік. Для аналізу результатів були застосовані: параметрична методологія статистики (ранговий аналіз) і непараметричні методи (поліхоричний аналіз), а також елементи фрактального аналізу. Результати. Встановлено, що найчастіше ДДК виникають у постраждалих вікової групи 41–50 років (33,70 %), найменше — у постраждалих старше 61 року (2,17 %). Загалом більшість постраждалих (81,53 %) становлять особи активного працездатного віку (21–50 років), що має важливе соціальне значення, оскільки ДДК мають великий ризик інвалідизації постраждалого. За клініко-анатомічним сегментом найчастіше ДДК у постраждалих виникають при пошкодженні нижніх кінцівок (86,96 %), причому ДДК гомілки становлять 67,39 %. Крім того, доведено, що існує вірогідна залежність виникнення ДДК за анатомічним сегментом у вікових групах. При аналізі показників дисипації за віковою ознакою та пошкодженим сегментом встановлено, що найбільший вплив на виникнення ДДК має вікова група 41–50 років та анатомічний сегмент «гомілка». Такий факт зумовлений як інволютивними змінами в організмі постраждалого, так і механізмом отримання пошкодження. Висновки. 1. Виникнення ДДК вірогідно залежить від вікової ознаки постраждалого та клініко-анатомічної ознаки пошкодження. 2. Найбільш часто ДДК виникають при пошкодженні гомілки і стегна й у віці 31–50 років, що відображає комбінований вплив інтенсивності ураження й інволютивного зменшення компенсаторних можливостей організму постраждалого. 3. Інтенсивність впливу вікових і клініко-анатомічних ознак є різною, причому найбільш інтенсивно впливають на виникнення ДДК ознака «гомілка» та вік 41–50 років. 4. Результати дослідження потребують подальшої клінічної інтерпретації з метою формування клініко-анатомічних, клініко-епідеміологічних і клінічних паралелей як основи для розробки клінічних протоколів і клінічних маршрутів пацієнта.
Background. Long bone defects (LBD) are usually the result of high-energy trauma and tend to spread among victims. Such pathology not only requires long-term treatment, but also leads to a high risk of disability, both due to the defect itself and possible amputation of the limb. Materials and methods. The study is cohort one and is based on the investigation and analysis of 92 cases of LBD of the limbs resulting from combat injuries sustained during military operations on the territory of Ukraine from 2022 to 2024. To analyze the results, the following methods were used: parametric statistical methodology (rank analysis) and non-parametric (polychoric analysis), as well as elements of fractal analysis. Results. It was found that LBD most frequently occur in patients aged 41–50 years (33.70 %), and least often in those over 61 years (2.17 %). In general, most victims (81.53 %) were individuals of active working age (21–50 years), which is of significant social importance, since LBD is associated with a high risk of disability. By clinical and anatomical segment, LBD were most often observed in lower limb injuries (86.96 %), with the LBD of the lower leg being 67.39 %. Furthermore, a significant dependence was found of the LBD occurrence by anatomical segment in age groups. Analysis of dissipation indices by age and injured segment revealed the age group of 41–50 years and the anatomical segment “lower leg” have the greatest influence on the occurrence of LBD. This fact is due to both involutive changes in the patients’ bodies and the mechanism of injury. Conclusions. 1. The occurrence of LBD probably depends on the age and the clinical and anatomical characteristics of the injury. 2. LBD most often occur with damage to the lower leg and at the age of 31–50 years, which reflects the combined effect of the severity of the lesion and the involutive decrease in the compensatory capabilities of the victim’s body. 3. The intensity of the impact of age and clinical and anatomical characteristics is different, with the “lower leg” characteristic and the age of 41–50 years having the most significant influence on the occurrence of LBD. 4. The results of the study require further clinical interpretation in order to form clinical and anatomical, clinical and epidemiological and clinical parallels as a basis for developing clinical protocols and clinical routes of the patient.
дефекти довгих кісток; клініко-анатомічна характеристика; вік; постраждалі
long bone defects; clinical and anatomical characteristics; age; victims