
Журнал "Гастроэнтерология" Том 59, №2, 2025
Вернуться к номеру
Порушення стравохідно-шлункової моторної функції як предиктор розвитку грижі стравохідного отвору діафрагми у військовослужбовців
Авторы: O.M. Babii, B.F. Shevchenko, N.V. Prolom, A.M. Halinska, О.О. Halinskyi
Institute of Gastroenterology of NAMSU, Dnipro, Ukraine
Рубрики: Гастроэнтерология
Разделы: Клинические исследования
Версия для печати
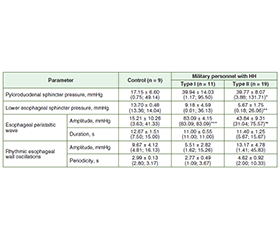
Актуальність. Порушення стравохідно-шлункової моторної функції, яка супроводжується розвитком грижі стравохідного отвору діафрагми (ГСОД), є поширеною патологією. Ці зміни можуть залежати від способу життя, рівня фізичного навантаження й адаптаційних механізмів, що відрізняються у військовослужбовців і цивільних. Оцінка таких відмінностей є важливою для розробки індивідуалізованих підходів до діагностики та лікування ГСОД. Мета: визначити порушення стравохідно-шлункової моторної функції як предиктора розвитку ГСОД у військовослужбовців шляхом аналізу показників цифрової пневмобалонної манометрії. Матеріали та методи. Проведено цифрову пневмобалонну манометрію стравоходу і шлунка в 66 пацієнтів із ГСОД (30 військовослужбовців і 36 цивільних (група порівняння)). Проаналізовано амплітуди й період перистальтичної хвилі, ритмічні коливання стінки стравоходу, тиск у зоні нижнього стравохідного сфінктера та пілородуоденального сфінктера. Результати. Амплітуда перистальтичної хвилі у військовослужбовців була в 1,9 раза вищою, ніж у цивільних, але період хвилі в цивільних був на 40,5 % довшим (p < 0,05). Ритмічні коливання стінки стравоходу в цивільних були менш вираженими, що може свідчити про більш значні порушення моторики. Тиск у зоні нижнього стравохідного сфінктера був знижений на 50,7 % у військових (p < 0,05) та на 53,7 % у цивільних (p < 0,01) порівняно з контролем, що призводило до розвитку гастроезофагеального рефлюксу. Тиск у зоні пілородуоденального сфінктера був підвищений відповідно у 2,2 і 2,8 раза у військовослужбовців та цивільних (p < 0,05). Висновки. Оцінка стравохідно-шлункової моторної функції за допомогою цифрової пневмобалонної манометрії дозволяє встановити предиктори розвитку ГСОД у військовослужбовців. Отримані результати вказують на необхідність персоналізованого підходу до лікування ГСОД.
Background. Disorders of esophagogastric motility, often associated with the development of hiatal hernia (HH), represent a common pathological condition. The characteristics of these functional changes may vary depending on lifestyle factors, levels of physical activity, and adaptive mechanisms, which differ between military personnel and civilians. Evaluation of such differences is essential for the development of individualized approaches to the diagnosis and treatment of HH. The purpose was to identify esophagogastric motility disorders as predictors of hiatal hernia development in military personnel by analyzing parameters obtained through digital pneumoballoon manometry. Materials and methods. Digital pneumoballoon manometry of the esophagus and stomach was performed in 66 patients with hiatal hernia (30 military personnel and 36 civilians, serving as the comparison group). The analysis included assessment of the amplitude and duration of peristaltic waves, rhythmic fluctuations of the esophageal wall, and pressure in the areas of the lower esophageal sphincter and pyloroduodenal sphincter. Results. The amplitude of the peristaltic wave in military personnel was 1.9 times higher than in civilians, whereas the wave duration in civilians was 40.5 % longer (p < 0.05). Rhythmic oscillations of the esophageal wall were less pronounced in civilians, suggesting more significant motility disorders. Pressure in the lower esophageal sphincter region was reduced by 50.7 % in military personnel (p < 0.05) and by 53.7 % in civilians (p < 0.01) compared to control values, contributing to the development of gastroesophageal reflux. Pressure in the pyloroduodenal sphincter region increased 2.2-fold in military personnel and 2.8-fold in civilians (p < 0.05). Conclusions. Assessment of esophagogastric motility using digital pneumoballoon manometry enables the identification of predictors of HH development in military personnel. The results underscore the need for a personalized approach to the treatment of hiatal hernia.
предиктори грижі стравохідного отвору діафрагми; стравохідно-шлункова моторна функція; тиск у зоні нижнього стравохідного сфінктера; тиск у зоні пілородуоденального сфінктера; функціональні дослідження
hiatal hernia predictors; esophagogastric motility; lower esophageal sphincter pressure; pyloroduodenal sphincter pressure; functional diagnosis
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Tack J, Pandolfino JE. Pathophysiology of gastroesophageal reflux disease. Gastroenterology. 2018;154(2):277-288. doi: 10.1053/j.gastro.2017.09.047.
- Fuchs KH, Meining A. Current insights in the pathophy–siology of gastroesophageal reflux disease. Chirurgia (Bucur). 2021;116(5):515-523. doi: 10.21614/chirurgia.116.5.515.
- Conrado LM, Gurski RR, da Rosa AR, Simic AP, Callegari-–Jacques SM. Is there an association between hiatal hernia and ineffective esophageal motility in patients with gastroesophageal reflux disease? J Gastrointest Surg. 2011;15(10):1756-1761. doi: 10.1007/s11605-011-1619-2.
- Stegerhoek P, Kooijman K, Ziesemer K, IJzerman H, Kuijer PPFM, Verhagen E. Risk factors for adverse health in military and law enforcement personnel; an umbrella review. BMC Public Health. 2024;24(1):3151. doi: 10.1186/s12889-024-20553-2.
- Shevchenko B, Prolom N, Babii O, Zeleniuk O, Tarabarov S, Galinsky O. Diagnosis and surgical correction of insufficiency of phy–siological cardia in hiatal hernia. Gastroenterology. 2022;56(1):48-53. doi: 10.22141/2308-2097.56.1.2022.487.
- Kayali S, Calabrese F, Pasta A, Marabotto E, Bodini G, et al. Effect of hiatal hernia and esophagogastric junction morphology on esopha–geal motility: evidence from high-resolution manometry stu–dies. Neurogastroenterol Motil. 2024;36(12):e14929. doi: 10.1111/nmo.14929.
- Hoshino M, Omura N, Yano F, Tsuboi K, Yamamoto SR, et al. Is esophageal manometry essential for the diagnosis of achalasia? Identifying patients with achalasia by the esophageal clearance method. Esophagus. 2021;18(1):163-168. doi: 10.1007/s10388-020-00756-3.
- Fox MR, Kahrilas PJ, Roman S, Gyawali CP, Scott SM, et al.; International Working Group for Disorders of Gastrointestinal Motility and Function. Clinical measurement of gastrointestinal motility and function: who, when and which test? Nat Rev Gastroenterol Hepatol. 2018;15(9):568-579. doi: 10.1038/s41575-018-0030-9.
- Akaishi T, Nakano T, Machida T, Abe M, Takayama S, et al. Clinical usefulness of endoscopy, barium fluoroscopy, and chest computed tomography for the correct diagnosis of achalasia. Intern Med. 2020;59(3):323-328. doi: 10.2169/internalmedicine.3612-19.
- Kahrilas PJ, Bredenoord AJ, Fox M, Gyawali CP, Roman S, Smout AJ, Pandolfino JE; International High Resolution Manometry Wor–king Group. The Chicago classification of esophageal motility disorders, v3.0. Neurogastroenterol Motil. 2015;27(2):160-174. doi: 10.1111/nmo.12477.
- Kahrilas PJ, Ghosh SK, Pandolfino JE. Esophageal motility disorders in terms of pressure topography: the Chicago classification. J Clin Gastroenterol. 2008;42(5):627-635. doi: 10.1097/MCG.0b013e31815ea291.
- Desipio J, Friedenberg FK, Korimilli A, Richter JE, Parkman HP, Fisher RS. High-resolution solid-state manometry of the antropyloroduodenal region. Neurogastroenterol Motil. 2007;19(3):188-195. doi: 10.1111/j.1365-2982.2006.00866.x.
- Siegal SR, Dolan JP, Hunter JG. Modern diagnosis and treatment of hiatal hernias. Langenbecks Arch Surg. 2017;402(8):1145-1151. doi: 10.1007/s00423-017-1606-5.
- Van Hoeij FB, Smout AJ, Bredenoord AJ. Predictive value of routine esophageal high-resolution manometry for gastro-esophageal reflux disease. Neurogastroenterol Motil. 2015;27(7):963-970. doi: 10.1111/nmo.12570.
- Severynovska OV, Galinskij OO, Rudenko AI, Mursin OB, Babicheva VV, Skubytska LD. Features of the gastric periodic acti–vity in conditions of NO-ergic system disbalance. Regul Mech Biosyst. 2014;5(1):71-78. doi: 10.15421/021415.