
Журнал «Травма» Том 26, №2, 2025
Вернуться к номеру
Захворюваність, смертність, причини раптової зупинки кровообігу: серцево-легенева реанімація у світі та реалії в Україні
Авторы: Чорна В.В. (1), Гудзевич Л.С. (2), Нестерова С.Ю. (2), Степаненко І.О. (2), Липкань В.М. (1, 3), Коломієць В.В. (1), Іщенко О.В. (1)
(1) - Вінницький національний медичний університет імені М.І. Пирогова, м. Вінниця, Україна
(2) - Вінницький державний педагогічний університет імені Михайла Коцюбинського, м. Вінниця, Україна
(3) - Військово-медичний клінічний центр Центрального регіону, м. Вінниця, Україна
Рубрики: Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
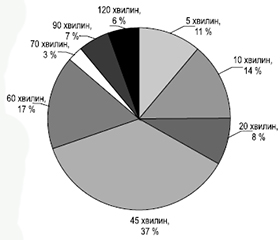
Мета дослідження полягала у проведенні аналізу офіційних даних Європейської ради реанімації у світі і в Україні щодо позалікарняної раптової зупинки кровообігу у військовослужбовців під час бойових дій з урахуванням причин, часу від поранення до початку проведення реанімаційних заходів, ускладнень за даними хірургічного госпіталю ІІ рівня (ІІ етап медичної евакуації (ЕМЕ)) ЗС України. Дослідження проводили на базі мобільного госпіталю (ЕМЕ ІІ рівня) найгарячішого напрямку бойових дій за червень — серпень 2024 р. Проаналізовано проведення реанімаційних заходів — серцево-легеневої реанімації на ЕМЕ ІІ рівня ЗС України в 36 військовослужбовців. Проведено ретроспективний огляд 86 вітчизняних та зарубіжних наукових праць з використанням баз даних PubMed і Google Scholar. Після проведення огляду статей та ознайомлення з їхніми повними текстами було відібрано 35 джерел щодо проведення серцево-легеневої реанімації в осіб з позалікарняною зупинкою кровообігу у світі загалом та під час воєнних конфліктів зокрема. Глибина пошуку охоплює період з 2004 по 2024 р. У роботі використано бібліосемантичний, системного аналізу, статистичний методи. Найбільш поширеними причинами позалікарняної зупинки кровообігу були: травма грудної клітки, зокрема вогнепальні поранення, що супроводжувалися розвитком гідро- та пневмотораксу, а також гемоперикарду (21,6 %), вогнепальні поранення, які спричинили масивні кровотечі (21,5 %), відрив нижніх кінцівок (20,5 %), торакоабдомінальні поранення (20,4 %), отруєння продуктами горіння (16,0 %). Тривалість проведення реанімаційних заходів при позалікарняній зупинці кровообігу становила 5 хвилин у 11,1 %, 10 хвилин — у 13,8 %, 20 хвилин — у 8,3 %, 45 хвилин — у 36,5 %, 60 хвилин — у 16,6 %, 70 хвилин — у 2,7 %, 90 хвилин — у 5,5 %, 120 хвилин — у 5,5 % постраждалих. Успішні реанімаційні заходи проведено у 63,9 % військовослужбовців, а у 36,1 % результат негативний. Висновки. У світі щорічна частота позалікарняної зупинки серця становить приблизно 50–60 випадків на 100 тисяч осіб, причому 72,0 % зупинок серця відбуваються вдома, 15,0 % — на робочому місці, а найчастішим механізмом є фібриляція шлуночків — 17 на 100 тисяч осіб протягом року.
The study aimed to analyze official data from the European Resuscitation Council on out-of-hospital sudden cardiac arrest worldwide and in Ukraine among military personnel during combat, considering the causes, duration from injury to the start of resuscitation, and complications according to the data from level II surgical hospital (stage II of medical evacuation) of the Armed Forces of Ukraine. The study was conducted at a mobile hospital (stage II of medical evacuation) in the most active combat zones during June-August 2024. The analysis of resuscitation measures was conducted — cardiopulmonary resuscitation for 36 military personnel at stage II of medical evacuation of the Armed Forces of Ukraine. A retrospective review of 86 domestic and foreign scientific papers was performed using the PubMed and Google Scholar databases. After reviewing the articles and familiarizing with their full texts, 35 sources on cardiopulmonary resuscitation in individuals with out-of-hospital cardiac arrest worldwide and during armed conflicts were selected. The search depth covered the period from 2004 to 2024. The bibliosemantic, systems analysis, and statistical methods were used in the work. The most common causes of out-of-hospital cardiac arrest were chest trauma, in particular gunshot wounds, accompanied by the development of hydro- and pneumothorax, as well as hemopericardium (21.6 %), gunshot wounds that caused massive bleeding (21.5 %), lower limb amputation (20.5 %), thoracoabdominal injuries (20.4 %), and poisoning by combustion products (16.0 %). The duration of resuscitation measures for out-of-hospital cardiac arrest was 5 minutes in 11.1 %, 10 minutes in 13.8 %, 20 minutes in 8.3 %, 45 minutes in 36.5 %, 60 minutes in 16.6 %, 70 minutes in 2.7 %, 90 minutes in 5.5 %, and 120 minutes in 5.5 % of cases. Successful resuscitation measures were carried out in 63.9 % of military personnel, and in 36.1 % the outcome was negative. Conclusions. Worldwide, the annual incidence of out-of-hospital cardiac arrest is approximately 50–60 cases per 100 thousand people, with 72.0 % of cardiac arrests occurring at home, 15.0 % at work, and the most common mechanism is ventricular fibrillation — 17 per 100 thousand people per year.
позалікарняна раптова зупинка кровообігу; серцево-легенева реанімація; військовослужбовці; травми грудної клітки, пов’язані з бойовими діями; ЕМЕ ІІ рівня
out-of-hospital sudden cardiac arrest; cardiopulmonary resuscitation; military personnel; combat-related chest injuries; stage II of medical evacuation