
Журнал «Травма» Том 26, №2, 2025
Вернуться к номеру
Коротка транспедикулярна фіксація вибухових переломів у ділянці грудопоперекового переходу під час згинання тулуба вперед: біомеханічне дослідження методом скінченних елементів
Авторы: Нехлопочин О.С. (1), Вербов В.В. (1), Чешук Є.В. (1), Карпінський М.Ю. (2), Яресько О.В. (2)
(1) - ДУ «Інститут нейрохірургії імені академіка А.П. Ромоданова НАМН України», м. Київ, Україна
(2) - ДУ «Інститут патології хребта та суглобів імені професора М.І. Ситенка НАМН України»,
м. Харків, Україна
Рубрики: Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
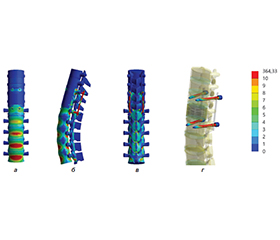
Актуальність. Травми грудопоперекового переходу (Th11–L2) становлять близько 46,5 % усіх переломів хребта. Вибухові переломи найчастіше трапляються саме в зоні переходу грудного кіфозу в поперековий лордоз, що зумовлено специфічними морфологічними та біомеханічними особливостями цієї ділянки. У хірургічній практиці простежується тенденція до застосування мінімально інвазивних технологій, зокрема короткої транспедикулярної фіксації, проте за нестабільних вибухових переломів такий підхід нерідко супроводжується підвищеним ризиком неспроможності металоконструкції. Мета: оцінити напружено-деформований стан моделей грудопоперекового відділу хребта з вибуховим переломом тіла хребця Th12 під час згинання тулуба вперед за різних варіантів короткої транспедикулярної фіксації (короткими й довгими гвинтами, з додатковою фіксацією хребця Th12 чи без неї). Матеріали та методи. Використано розроблену скінченно-елементну 3D-модель грудопоперекового відділу хребта із вибуховим переломом тіла Th12. Моделювали чотири варіанти транспедикулярної фіксації двох суміжних з ушкодженим хребців: із короткими й довгими гвинтами, які проходять крізь передню поверхню тіла хребця, а також додатковими двома короткими гвинтами в тіло Th12 та без них. Імітували нахил тулуба вперед за жорсткого закріплення нижньої поверхні диска L5. Напруження за Мізесом визначали в низці контрольних точок. Результати. Встановлено, що без додаткової фіксації Th12 використання довгих гвинтів, порівняно з короткими, забезпечує нижчі пікові напруження в тілі хребця Th12, сусідніх хребцях і металоконструкції. Максимальні напруження на гвинтах та опорних балках лишаються доволі високими, проте відчутно зменшуються під час застосування довгих гвинтів. Використання проміжних гвинтів істотно знижує напруження в кісткових елементах, що важливо для профілактики розхитування й міграції гвинтів. Поєднання довгих гвинтів із додатковою фіксацією Th12 виявилося найбільш ефективним для мінімізації напружень у кісткових структурах і металоконструкції. Висновки. Застосування короткої транспедикулярної фіксації разом із додатковою фіксацією Th12 суттєво зменшує рівень напружень у кісткових елементах, однак здатне викликати надмірне навантаження на фіксувальні елементи. Найоптимальнішим за показниками розподілу напружень (як у кісткових структурах, так і в металоконструкції) є комбінація довгих гвинтів із додатковою фіксацією Th12.
Background. Injuries to the thoracolumbar junction (T11-L2) account for approximately 46.5 % of all spinal fractures. Burst fractures most frequently occur at the transition from thoracic kyphosis to lumbar lordosis, which is influenced by the distinct morphological and biomechanical features of this region. In surgical practice, there is a trend toward minimally invasive techniques, including short transpedicular fixation, yet in cases of unstable burst fractures, this approach often carries a high risk of hardware failure. Objective: to evaluate the stress-strain state of thoracolumbar spine models with a burst fracture of the T12 vertebral body during forward bending under different variants of short transpedicular fixation (short or long screws, with or without additional fixation of T12). Materials and methods. A previously developed finite element 3D model of the thoracolumbar spine with a burst fracture of the T12 vertebral body was used. Four variants of transpedicular fixation of the two vertebrae adjacent to the injury were modeled: with short and long screws passing through the anterior vertebral wall, as well as an additional pair of short screws inserted into T12 or without them. A forward-bending movement was simulated, while the lower surface of the L5 disc was fixed. Von Mises stress was evaluated at several control points. Results. Without additional T12 fixation, using long screws (as opposed to short one) lowered the peak stresses in the T12 body, adjacent vertebrae, and instrumentation. Although the highest stress levels on the screws and support beams remained significant, they were noticeably reduced with long screws. Using intermediate screws considerably decreased stress in the bony elements, which is important for preventing screw loosening and migration. Combining long screws with additional T12 fixation proved to be most effective in minimizing stress in both bony structures and the instrumentation. Conclusions. Short transpedicular fixation with additional T12 fixation substantially lowers stress levels in the vertebrae but can lead to excessive loading on hardware components. The most favorable option for stress distribution in both the bony structures and the instrumentation is the combination of long screws and additional T12 fixation.
грудопоперековий перехід; вибуховий перелом; коротка транспедикулярна фіксація; метод скінченних елементів; біомеханічний аналіз, напружено-деформований стан, флексійне навантаження
thoracolumbar junction; burst fracture; short transpedicular fixation; finite element method; biomechanical analysis; stress-strain state; flexion load