
Журнал «Здоровье ребенка» Том 19, №2, 2024
Вернуться к номеру
Особливості діагностики неповної форми хвороби Кавасакі у дітей раннього віку. Клінічний випадок хвороби Кавасакі із формуванням гігантських аневризм коронарних артерій
Авторы: Мальська А.А. (1), Куриляк О.Б. (2), Наконечна Л.М. (2), Климишин Ю.І. (3), Стогова О.В. (3), Таммо Раад (3), Руденко Н.М. (4)
(1) - Львівський національний медичний університет імені Данила Галицького, м. Львів, Україна
(2) - КНП ЛОР «Львівська обласна дитяча клінічна лікарня «ОХМАТДИТ», Центр дитячої медицини, м. Львів, Україна
(3) - ДУ «НПМ «Центр дитячої кардіології та кардіохірургії» МОЗ України, м. Київ, Україна
(4) - Національний університет охорони здоров’я України імені П.Л. Шупика, м. Київ, Україна
Рубрики: Педиатрия/Неонатология
Разделы: Справочник специалиста
Версия для печати
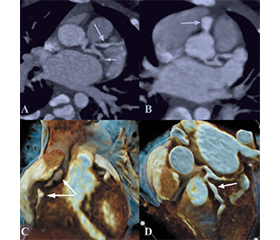
Хвороба Кавасакі (ХК) — слизово-шкірний лімфонодулярний синдром, це васкуліт невідомої етіології, який переважно вражає дітей віком до 5 років. На сьогодні ХК є найпоширенішою причиною набутих патологій серця у дітей у розвинених країнах. З огляду на відсутність патогномонічної діагностики захворювання, діагноз ґрунтується виключно на визначенні клінічних ознак та виключенні інших клінічно подібних захворювань. Своєчасна терапія внутрішньовенним імуноглобуліном значно знизила частоту розвитку ускладнень — аневризм коронарних артерій з 25 до ≈ 4 %. Довгостроковий прогноз захворювання залежить від початкового та поточного рівня ураження коронарних артерій. У пацієнтів з аневризмами коронарних артерій залишається високий ризик розвитку ішемії міокарда внаслідок тромбозу та стенозу коронарних артерій, що можуть виникнути при несвоєчасному лікуванні ХК, відтак життя цих пацієнтів залежить від пожиттєвої тромбопрофілактики та вчасної діагностики стенозів. У статті наведено клінічний випадок утрудненої діагностики неповної форми хвороби Кавасакі, яка ускладнилась розвитком гігантських аневризм коронарних артерій.
Kawasaki disease (KD) is a mucocutaneous lymphonodular syndrome, a vasculitis of unknown etiology that mainly affects children under the age of 5 years. Today, KD is the most common cause of acquired heart disease in children in developed countries. Given the absence of pathognomonic diagnosis of the disease, the diagnosis is based solely on the identification of clinical signs and the exclusion of other clinically similar diseases. Timely therapy with intravenous immunoglobulin has significantly reduced the incidence of complications, such as coronary artery aneurysms, from 25 to ≈ 4 %. The long-term prognosis of the disease depends on the initial and current level of coronary artery damage. Patients with coronary artery aneurysms remain at high risk of developing myocardial ischaemia due to thrombosis and stenosis of the coronary arteries, which can occur in case of untimely treatment for KD. Therefore, the life of these patients depends on lifelong thromboprophylaxis and timely diagnosis of stenosis. The article presents a clinical case of incomplete Kawasaki disease, which was complicated by the development of giant coronary artery aneurysms.
хвороба Кавасакі; аневризми коронарних артерій; ураження серця; лихоманка; діти раннього віку
Kawasaki disease; coronary artery aneurysms; heart lesions; fever; young children
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Miura M., Ayusawa M., Fukazawa R., Hamada H., Ikeda S., Ito S., et al. Guidelines for Medical Treatment of Acute Kawasaki Disease (2020 Revised Version). Journal of Pediatric Cardiology and Cardiac Surgery. 2021. 5. Iss. 1. 41-73. Released on J-STAGE July 10, 2021, https://doi.org/10.24509/jpccs.0501G1, https://www.jstage.jst.go.jp/article/jpccs/5/1/5_0501G1/_article/-char/en.
- Maddox R.A., Holman R.C., Uehara R., Callinan L.S., Guest J.L., Schonberger L.B., et al. Recurrent Kawasaki disease: USA and Japan. Pediatr. Int. 2015. 57. 1116-1120. doi: 10.1111/ped.12733.
- Kobayashi T., Ayusawa M., Suzuki H., Abe J., Ito S., Kato T., et al. Revision of diagnostic guidelines for Kawasaki disease (6th revised edition). Pediatrics International. 2020. 62. 1135-1138. https://doi.org/10.1111/ped.14326.
- de Graeff N., Groot N., Ozen S., Eleftheriou D., Avcin T., Bader-Meunier B., et al. European consensus-based recommendations for the diagnosis and treatment of Kawasaki disease — the SHARE initiative, Rheumatology. 2019 April. 58. Is. 4. 672-682; https://doi.org/10.1093/rheumatology/key344.
- Klymyshyn Y., Datsko O., Stepanovskyy Yu., Nagao Y., Nagayama Y., Ueno S., et al. A Ukrainian infant with giant coronary aneurysms: A case report and literature review. Clinical Case Reports. 2023. 11. Iss. 5.
- Wessels P.A., Bingler M.A. A comparison of Kawasaki Disease and multisystem inflammatory syndrome in children. Prog. Pediatr. Cardiol. 2022 Jun. 65. 101516. doi: 10.1016/j.ppedcard.2022.101516. Epub 2022 Mar 16. PMID: 35313700; PMCID: PMC8925196.
- Printz B.F., Sleeper L.A., Newburger J.W., Minich L.L., Bradley T., Cohen M.S., et al.; Pediatric Heart Network Investigators. Noncoronary cardiac abnormalities are associated with coronary artery dilation and with laboratory inflammatory markers in acute Kawasaki disease. J. Am. Coll. Cardiol. 2011. 57. 86-92. doi: 10.1016/j.jacc.2010.08.619.
- Dengler L.D., Capparelli E.V., Bastian J.F., Bradley D.J., Glode M.P., Santa S., et al. Cerebrospinal fluid profile in patients with acute Kawasaki disease. Pediatr. Infect. Dis. J. 1998. 17. 478-481.
- Poon L.K., Lun K.S., Ng Y.M. Facial nerve palsy and Kawasaki disease. Hong Kong Med. J. 2000. 6. 224-226.
- Alves N.R., Magalhães C.M., Almeida Rd.F.R., Santos R.C., Gandolfi L., Pratesi R. Prospective study of Kawasaki disease complications: review of 115 cases. Rev. Assoc. Med. Bras. 1992. 2011. 57. 295-300.
- Baker A.L., Lu M., Minich L.L., Atz A.M., Klein G.L., Korsin R., et al.; Pediatric Heart Network Investigators. Associated symptoms in the ten days before diagnosis of Kawasaki disease. J. Pediatr. 2009. 154. 592-595.e2. doi: 10.1016/j.jpeds.2008.10.006.
- Uehara R., Igarashi H., Yashiro M., Nakamura Y., Yanagawa H. Kawasaki disease patients with redness or crust formation at the Bacille Calmette-Guérin inoculation site. Pediatr. Infect. Dis. J. 2010. 29. 430-433. doi: 10.1097/INF.0b013e3181cacede.
- Minich L.L., Sleeper L.A., Atz A.M., McCrindle B.W., Lu M., Colan S.D., et al.; Pediatric Heart Network Investigators. Delayed diagnosis of Kawasaki disease: what are the risk factors? Pediatrics. 2007. 120. e1434-e1440. doi: 10.1542/peds.2007-0815. Crossref. PubMed.
- McCrindle B.W., Rowley A.H., Newburger J.W., Burns J.C., Bolger, Gewitz M., et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific St A.F.atement for Health Professionals From the American Heart Association. Originally published 29 Mar 2017; https://doi.org/10.1161/CIR.0000000000000484. Circulation. 2017. 135. e927-e999.
- Takahashi K., Oharaseki T., Yokouchi Y., Yamada H., Shibuya K., Naoe S. A half-century of autopsy results-incidence of pediatric vasculitis syndromes, especially Kawasaki disease. Circ. J. 2012. 76. 964-970.
- Lin K.H., Chang S.S., Yu C.W., Lin S.C., Liu S.C., Chao H.Y., et al. Usefulness of natriuretic peptide for the diagnosis of Kawasaki disease: a systematic review and meta-analysis. BMJ Open. 2015. 5. e006703. doi: 10.1136/bmjopen-2014-006703.
- Sumitomo N., Karasawa K., Taniguchi K., Ichikawa R., Fukuhara J., Abe O., et al. Association of sinus node dysfunction, atrioventricular node conduction abnormality and ventricular arrhythmia in patients with Kawasaki disease and coronary involvement. Circ. J. 2008. 72. 274-280.
- Burns J.C., Franco A. The immunomodulatory effects of intravenous immunoglobulin therapy in Kawasaki disease. Expert Rev. Clin. Immunol. 2015. 11. 819-825. doi: 10.1586/1744666X.2015.1044980.
- Oates-Whitehead R.M., Baumer J.H., Haines L., Love S., Maconochie I.K., Gupta A., et al. Intravenous immunoglobulin for the treatment of Kawasaki disease in children. Cochrane Database Syst. Rev. 2003. (4). CD004000.
- Manlhiot C., Millar K., Golding F., McCrindle B.W. Improved classification of coronary artery abnormalities based only on coronary artery z-scores after Kawasaki disease. Pediatr. Cardiol. 2010. 31. 242-249. doi: 10.1007/s00246-009-9599-7.
- Terai M., Shulman S.T. Prevalence of coronary artery abnormalities in Kawasaki disease is highly dependent on gamma globulin dose but independent of salicylate dose. J. Pediatr. 1997. 131. 888-893.
- Baumer J.H., Love S.J., Gupta A., Haines L.C., Maconochie I., Dua J.S. Salicylate for the treatment of Kawasaki disease in children. Cochrane Database Syst. Rev. 2006. (4). CD004175.